

SARS-CoV-2 booster vaccination rescues attenuated IgG1 memory B cell response in primary antibody deficiency patients
- PMID: 36618402
- PMCID: PMC9817149
- DOI: 10.3389/fimmu.2022.1033770
SARS-CoV-2 booster vaccination rescues attenuated IgG1 memory B cell response in primary antibody deficiency patients
Abstract
Background: Although SARS-CoV-2 vaccines have proven effective in eliciting a protective immune response in healthy individuals, their ability to induce a durable immune response in immunocompromised individuals remains poorly understood. Primary antibody deficiency (PAD) syndromes are among the most common primary immunodeficiency disorders in adults and are characterized by hypogammaglobulinemia and impaired ability to mount robust antibody responses following infection or vaccination.
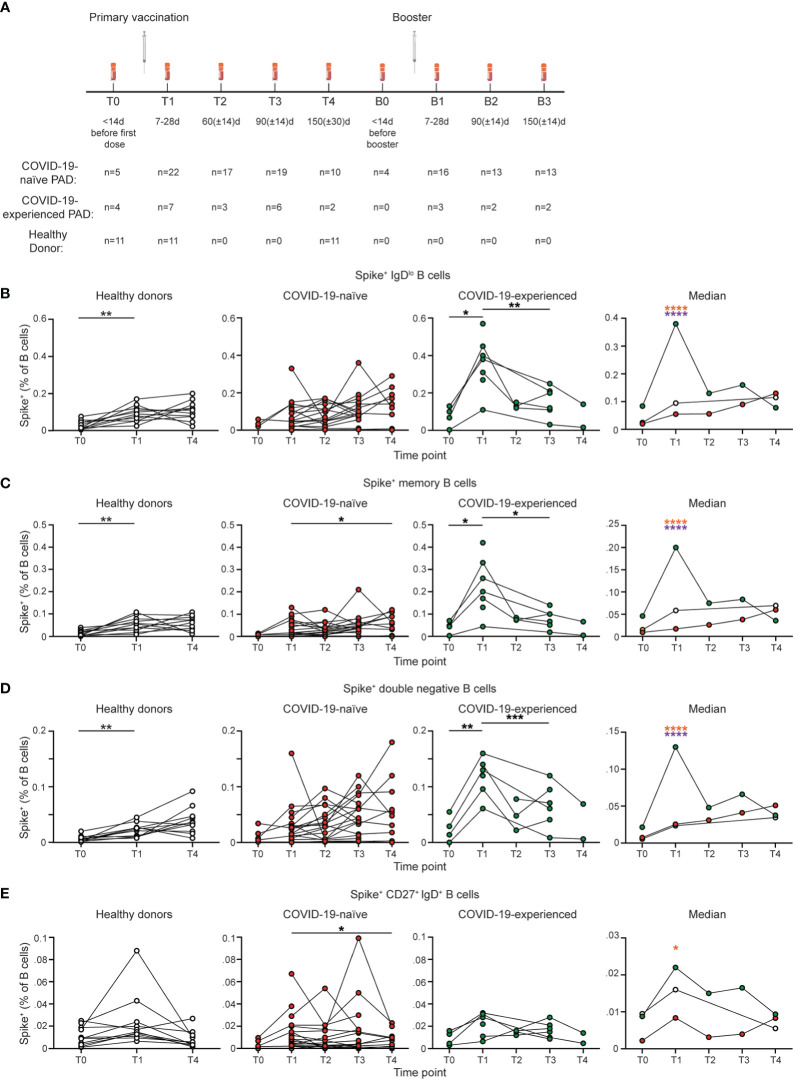
Methods: Here, we present an analysis of both the B and T cell response in a prospective cohort of 30 individuals with PAD up to 150 days following initial COVID-19 vaccination and 150 days post mRNA booster vaccination.
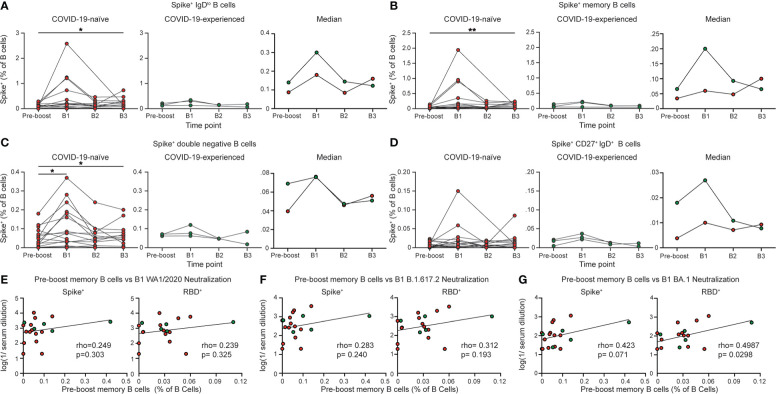
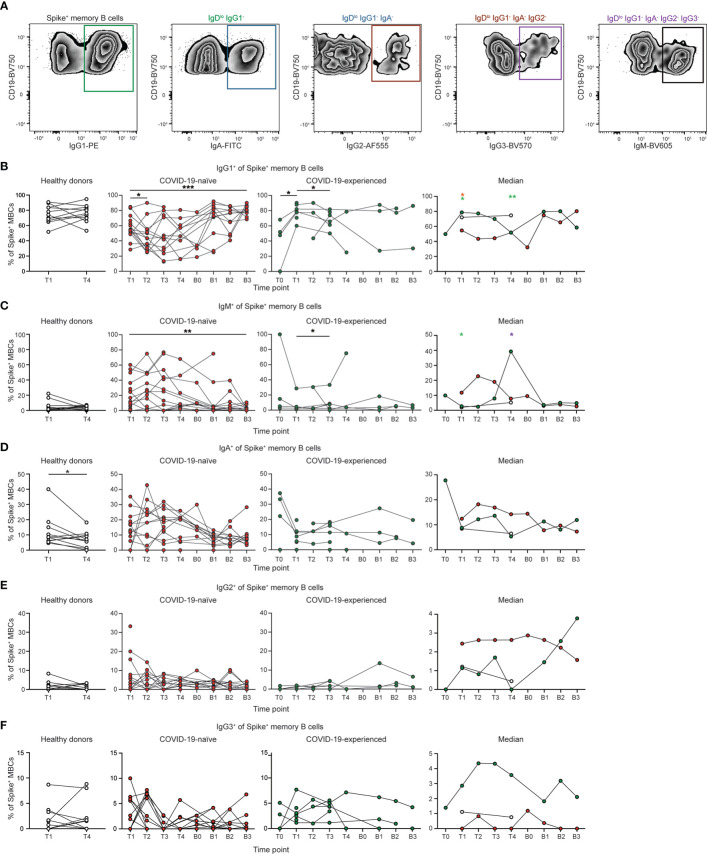
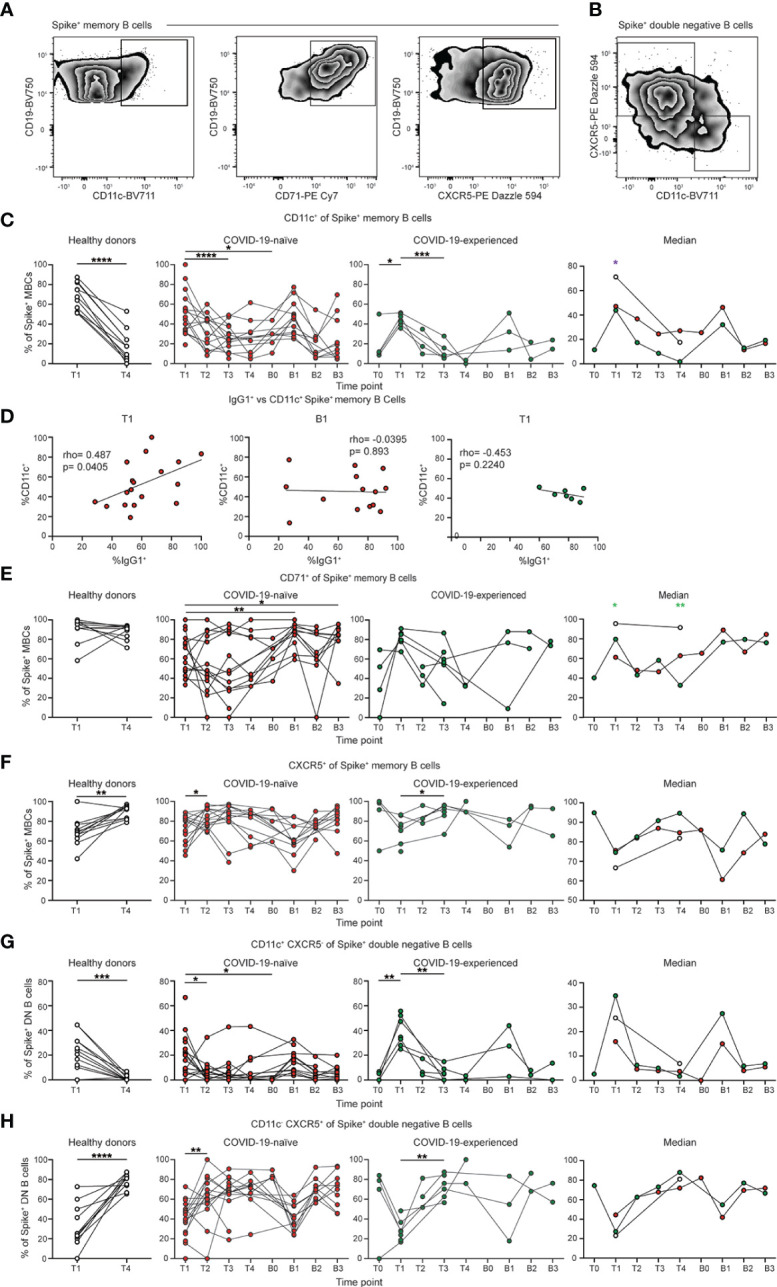
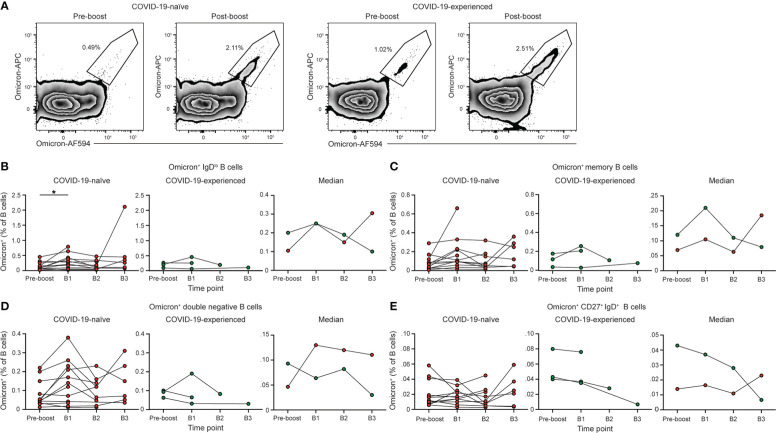
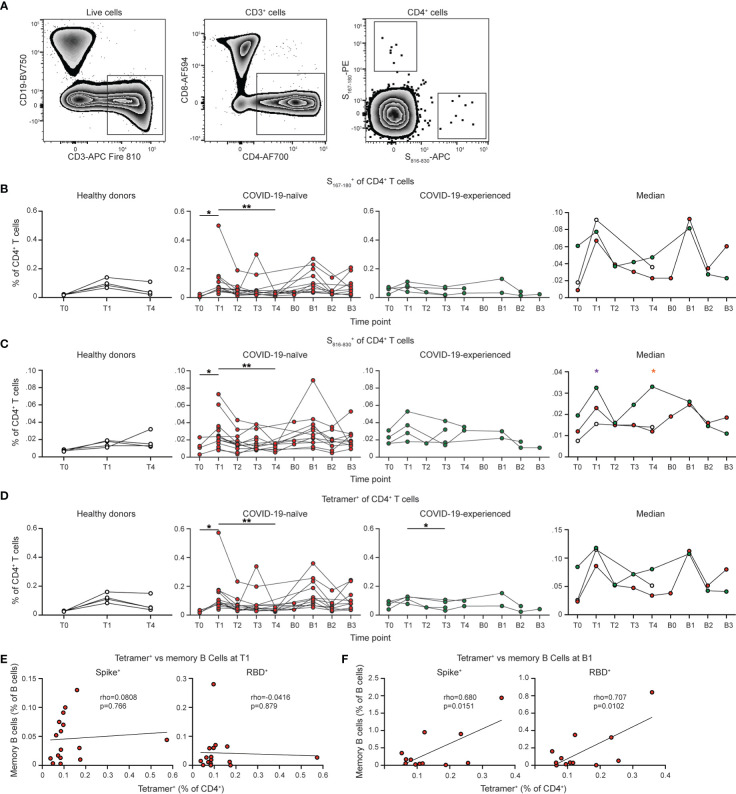
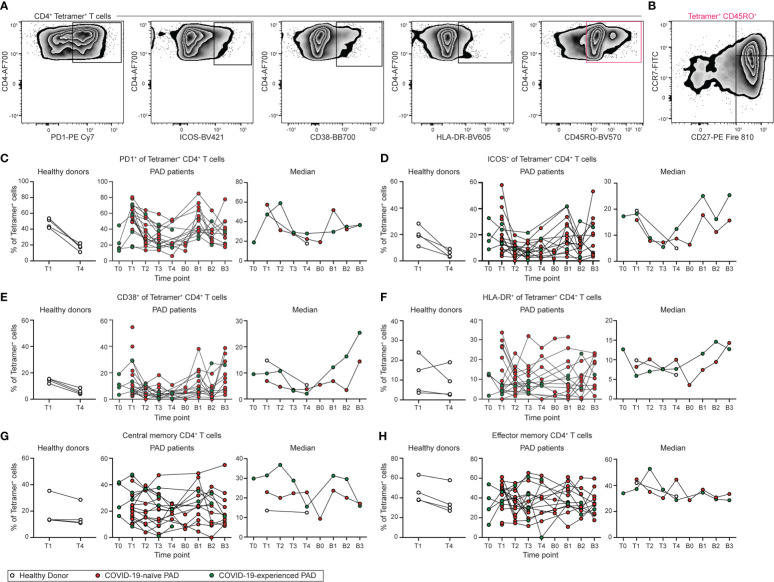
Results: After the primary vaccination series, many of the individuals with PAD syndromes mounted SARS-CoV-2 specific memory B and CD4+ T cell responses that overall were comparable to healthy individuals. Nonetheless, individuals with PAD syndromes had reduced IgG1+ and CD11c+ memory B cell responses following the primary vaccination series, with the defect in IgG1 class-switching rescued following mRNA booster doses. Boosting also elicited an increase in the SARS-CoV-2-specific B and T cell response and the development of Omicron-specific memory B cells in COVID-19-naïve PAD patients. Individuals that lacked detectable B cell responses following primary vaccination did not benefit from booster vaccination.
Conclusion: Together, these data indicate that SARS-CoV-2 vaccines elicit memory B and T cells in most PAD patients and highlights the importance of booster vaccination in immunodeficient individuals.
Keywords: B cells; SARS-CoV-2; common variable immunodeficiency; hypogammaglobulinemia; immune memory; primary antibody deficiency; specific antibody deficiency; vaccination.
Copyright © 2022 Lin, Doss, Davis-Adams, Adams, Hanson, VanBlargan, Liang, Chen, Monroy, Wedner, Kulczycki, Mantia, O’Shaughnessy, Raju, Zhao, Rizzi, Rigell, Dy, Kau, Ren, Turner, O’Halloran, Presti, Fremont, Kendall, Ellebedy, Mudd, Diamond, Zimmerman and Laidlaw.
Conflict of interest statement
MD is a consultant for Inbios, Vir Biotechnology, Senda Biosciences, Moderna, and Immunome. The Diamond laboratory has received unrelated funding support in sponsored research agreements from Moderna, Vir Biotechnology, Immunome, and Emergent BioSolutions. OZ and family own Moderna stock. The Ellebedy laboratory received unrelated funding support from Emergent BioSolutions and AbbVie. AE is a consultant for Mubadala Investment Company and the founder of ImmuneBio Consulting. JT is a consultant for Gerson Lehrman Group. JT and AE are recipients of a licensing agreement with Abbvie that is unrelated to this manuscript. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Cellular immune response to SARS-CoV-2 in patients with primary antibody deficiencies.Front Immunol. 2023 Oct 12;14:1275892. doi: 10.3389/fimmu.2023.1275892. eCollection 2023. Front Immunol. 2023. PMID: 37901210 Free PMC article.
-
Waning of specific antibodies against Delta and Omicron variants five months after a third dose of BNT162b2 SARS-CoV-2 vaccine in elderly individuals.Front Immunol. 2022 Nov 14;13:1031852. doi: 10.3389/fimmu.2022.1031852. eCollection 2022. Front Immunol. 2022. PMID: 36451833 Free PMC article.
-
Ancestral SARS-CoV-2 and Omicron BA.5-specific neutralizing antibody and T-cell responses after Omicron bivalent booster vaccination in previously infected and infection-naive individuals.J Med Virol. 2023 Aug;95(8):e28989. doi: 10.1002/jmv.28989. J Med Virol. 2023. PMID: 37565645
-
SARS-CoV-2 vaccination in primary antibody deficiencies: an overview on efficacy, immunogenicity, durability of immune response and safety.Curr Opin Allergy Clin Immunol. 2024 Feb 1;24(1):37-43. doi: 10.1097/ACI.0000000000000955. Epub 2023 Nov 14. Curr Opin Allergy Clin Immunol. 2024. PMID: 37962877 Review.
-
Profiling the B cell immune response elicited by vaccination against the respiratory virus SARS-CoV-2.Front Immunol. 2022 Nov 24;13:1058748. doi: 10.3389/fimmu.2022.1058748. eCollection 2022. Front Immunol. 2022. PMID: 36505416 Free PMC article. Review.
Cited by
-
Causal association of immune cells and endometritis: a Mendelian randomization study.Sci Rep. 2024 Oct 22;14(1):24822. doi: 10.1038/s41598-024-75827-x. Sci Rep. 2024. PMID: 39438592 Free PMC article.
-
The immunologic outcomes and adverse events of COVID-19 vaccine booster dose in immunosuppressed people: A systematic review.Prev Med Rep. 2024 May 31;44:102778. doi: 10.1016/j.pmedr.2024.102778. eCollection 2024 Aug. Prev Med Rep. 2024. PMID: 38979481 Free PMC article. Review.
-
An Overview of the Strategies to Boost SARS-CoV-2-Specific Immunity in People with Inborn Errors of Immunity.Vaccines (Basel). 2024 Jun 18;12(6):675. doi: 10.3390/vaccines12060675. Vaccines (Basel). 2024. PMID: 38932404 Free PMC article. Review.
-
Impact of Exposure to Vaccination and Infection on Cellular and Antibody Response to SARS-CoV-2 in CVID Patients Through COVID-19 Pandemic.J Clin Immunol. 2023 Dec 22;44(1):12. doi: 10.1007/s10875-023-01616-2. J Clin Immunol. 2023. PMID: 38129351
References
-
- Organization WH . WHO coronavirus (COV-19) dashboard (2022). Available at: https://covid19.who.int/ (Accessed August 18, 2022).
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous