

Theranostic Applications of Glycosaminoglycans in Metastatic Renal Cell Carcinoma
- PMID: 36612261
- PMCID: PMC9818616
- DOI: 10.3390/cancers15010266
Theranostic Applications of Glycosaminoglycans in Metastatic Renal Cell Carcinoma
Abstract
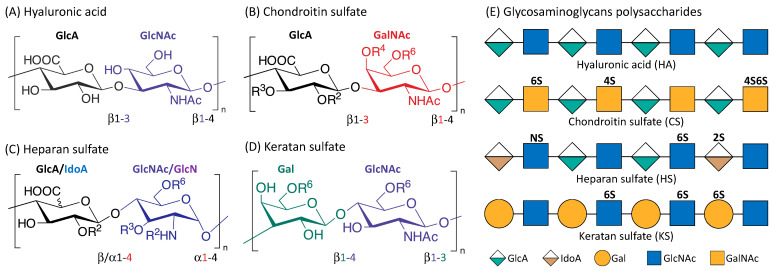
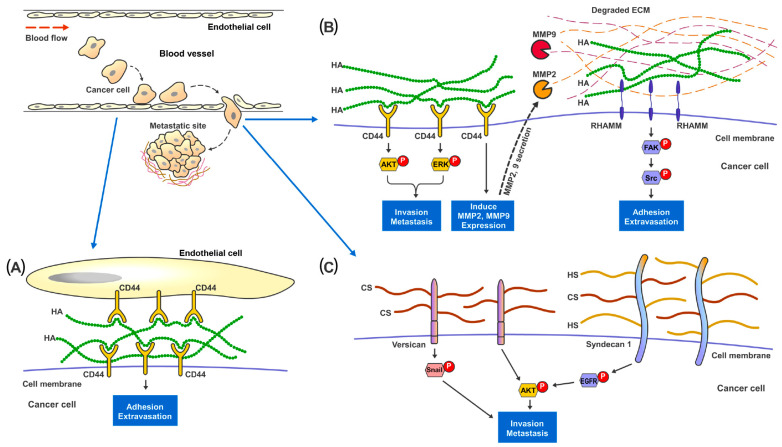
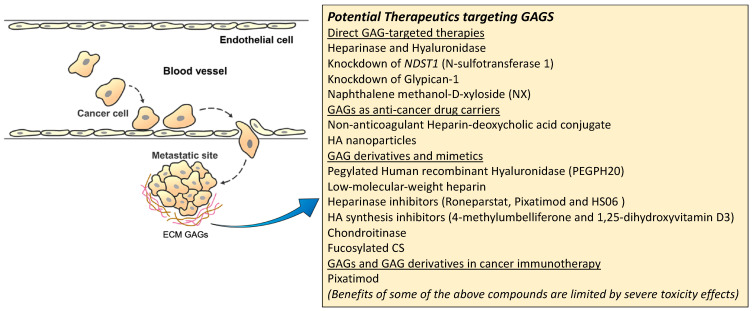
Renal cell carcinoma (RCC) makes up the majority of kidney cancers, with a poor prognosis for metastatic RCC (mRCC). Challenges faced in the management of mRCC, include a lack of reliable prognostic markers and biomarkers for precise monitoring of disease treatment, together with the potential risk of toxicity associated with more recent therapeutic options. Glycosaminoglycans (GAGs) are a class of carbohydrates that can be categorized into four main subclasses, viz., chondroitin sulfate, hyaluronic acid, heparan sulfate and keratan sulfate. GAGs are known to be closely associated with cancer progression and modulation of metastasis by modification of the tumor microenvironment. Alterations of expression, composition and spatiotemporal distribution of GAGs in the extracellular matrix (ECM), dysregulate ECM functions and drive cancer invasion. In this review, we focus on the clinical utility of GAGs as biomarkers for mRCC (which is important for risk stratification and strategizing effective treatment protocols), as well as potential therapeutic targets that could benefit patients afflicted with advanced RCC. Besides GAG-targeted therapies that holds promise in mRCC, other potential strategies include utilizing GAGs as drug carriers and their mimetics to counter cancer progression, and enhance immunotherapy through binding and transducing signals for immune mediators.
Keywords: biomarkers; glycosaminoglycans; metastasis; renal cell carcinoma; targeted therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Glycosaminoglycans: Carriers and Targets for Tailored Anti-Cancer Therapy.Biomolecules. 2021 Mar 8;11(3):395. doi: 10.3390/biom11030395. Biomolecules. 2021. PMID: 33800172 Free PMC article. Review.
-
Matrix glycosaminoglycans in the growth phase of fibroblasts: more of the story in wound healing.J Surg Res. 2000 Jul;92(1):45-52. doi: 10.1006/jsre.2000.5840. J Surg Res. 2000. PMID: 10864481
-
Glycosaminoglycans in cancer therapy.Am J Physiol Cell Physiol. 2022 Jun 1;322(6):C1187-C1200. doi: 10.1152/ajpcell.00063.2022. Epub 2022 Apr 6. Am J Physiol Cell Physiol. 2022. PMID: 35385322 Review.
-
Glycosaminoglycans: Sweet as Sugar Targets for Topical Skin Anti-Aging.Clin Cosmet Investig Dermatol. 2021 Sep 14;14:1227-1246. doi: 10.2147/CCID.S328671. eCollection 2021. Clin Cosmet Investig Dermatol. 2021. PMID: 34548803 Free PMC article. Review.
-
Bench-to-bedside review: the role of glycosaminoglycans in respiratory disease.Crit Care. 2006;10(6):237. doi: 10.1186/cc5069. Crit Care. 2006. PMID: 17118216 Free PMC article. Review.
Cited by
-
The Landscape of Small Leucine-Rich Proteoglycan Impact on Cancer Pathogenesis with a Focus on Biglycan and Lumican.Cancers (Basel). 2023 Jul 9;15(14):3549. doi: 10.3390/cancers15143549. Cancers (Basel). 2023. PMID: 37509212 Free PMC article. Review.
-
Revisiting the Syndecans: Master Signaling Regulators with Prognostic and Targetable Therapeutic Values in Breast Carcinoma.Cancers (Basel). 2023 Mar 16;15(6):1794. doi: 10.3390/cancers15061794. Cancers (Basel). 2023. PMID: 36980680 Free PMC article. Review.
-
High-throughput glycosaminoglycan extraction and UHPLC-MS/MS quantification in human biofluids.Nat Protoc. 2024 Nov 14. doi: 10.1038/s41596-024-01078-9. Online ahead of print. Nat Protoc. 2024. PMID: 39543382 Review.
-
Computational approach for assessing the involvement of SMYD2 protein in human cancers using TCGA data.J Genet Eng Biotechnol. 2023 Nov 16;21(1):122. doi: 10.1186/s43141-023-00594-7. J Genet Eng Biotechnol. 2023. PMID: 37971632 Free PMC article.
-
Teaching an Old Drug a New Trick: Targeting Treatment Resistance in Genitourinary Cancers.J Cell Signal. 2024;5(2):51-56. doi: 10.33696/signaling.5.112. J Cell Signal. 2024. PMID: 38726221 Free PMC article.
References
-
- Surveillance E., Program E.R. SEER Stat Fact Sheets: Kidney and Renal Pelvis Cancer. National Cancer Institute; Bethesda, MD, USA: 2017.
-
- Kosary C. Kidney and renal pelvis. SEER Cancer Statistics Review, 1973–1990. National Cancer Institute; Bethesda, MD, USA: 1993.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
