

Platelet-rich fibrin vs. buccal advancement flap for closure of oroantral communications: a prospective clinical study
- PMID: 36607489
- PMCID: PMC10264294
- DOI: 10.1007/s00784-022-04846-7
Platelet-rich fibrin vs. buccal advancement flap for closure of oroantral communications: a prospective clinical study
Abstract
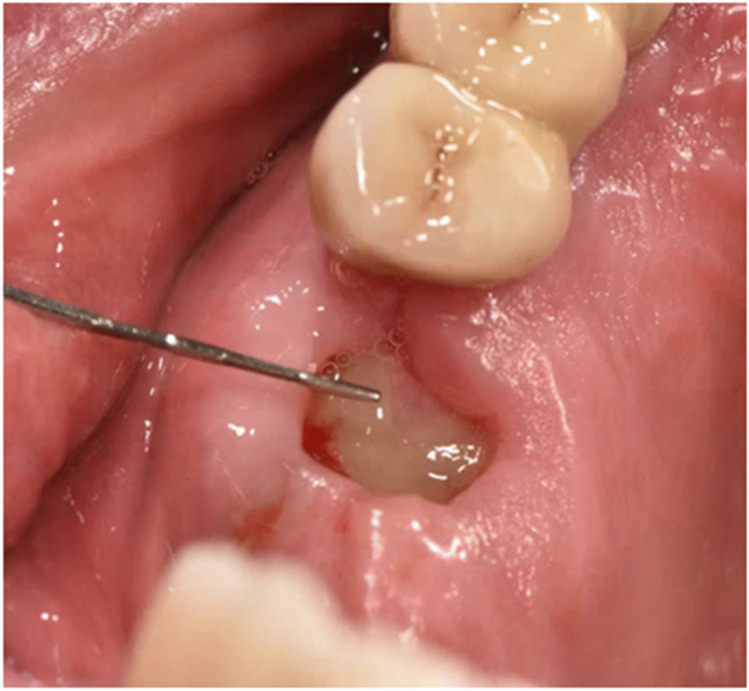
Objectives: The primary aim was to evaluate the success of the defect closure (tight or open) of oroantral communications (OAC) after treatment with platelet-rich fibrin (PRF) clots or a buccal advancement flap (BAF). Secondary outcome measurements were the evaluation of the wound healing, the displacement of the mucogingival border (MGB), and the pain level.
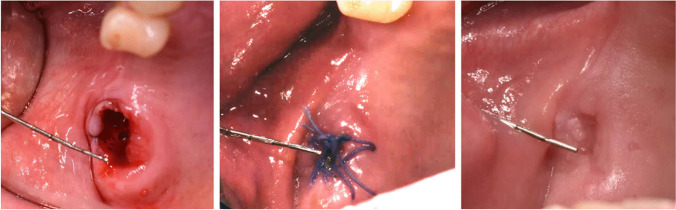
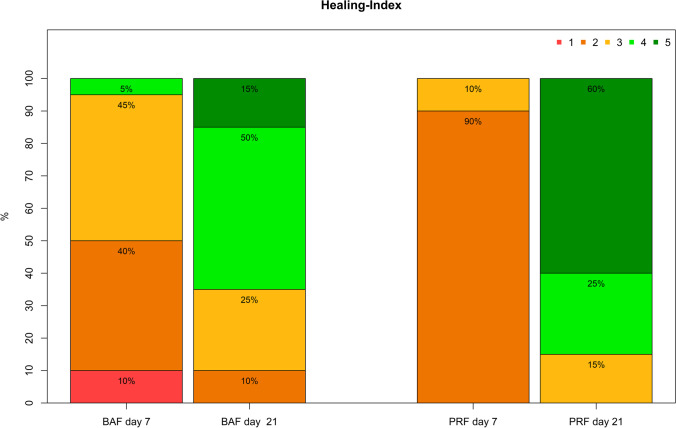
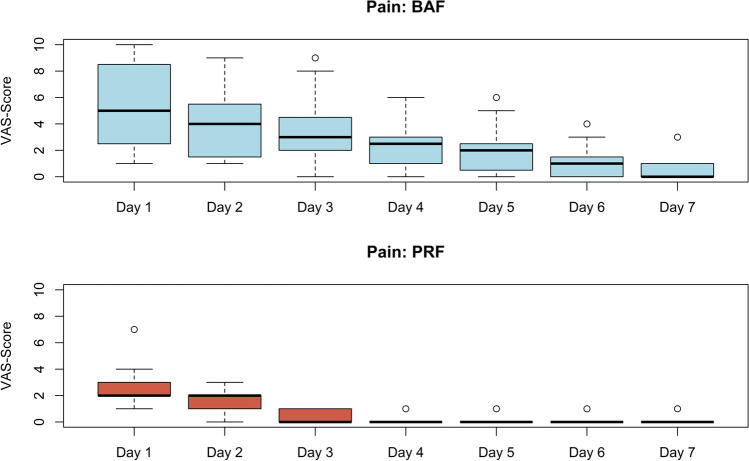
Material and methods: Fifty eligible patients with an OAC defect larger than 3 mm were randomly assigned to either PRF (test group, n = 25) or BAF (control group, n = 25) for defect closure. In a prospective follow-up program of 21 days, the defect closure healing process, the wound healing course using Landry's wound healing index (score: 0-5), the displacement of the MGB, and the postoperative pain score were evaluated.
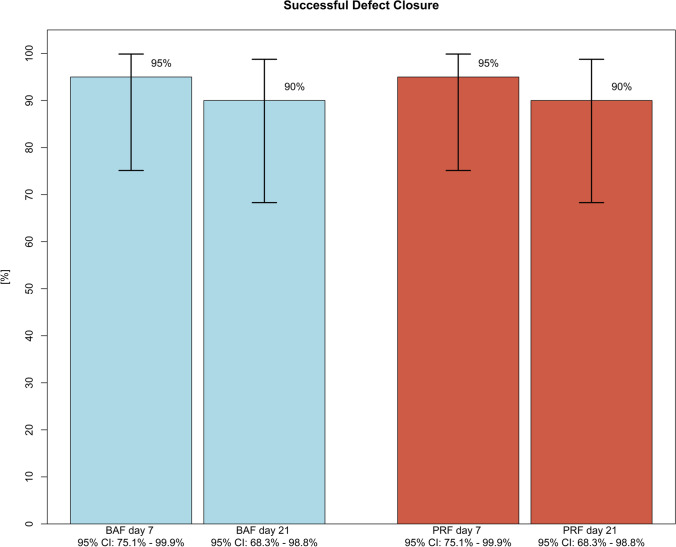
Results: Five patients in each group were lost to follow-up resulting in 40 patients (20 in each group) for continuous evaluation. On postoperative day 21 (study endpoint), no difference regarding success rate (defined as closure of OAC) was noticed between the test (90%; 18/20) and control group (90%; 18/20). A univariate analysis showed significant differences for age and defect size/height for the use of PRF between successful-tight and open-failed defect healing. At the final evaluation, a significantly (p = 0.005) better wound healing score, a lower displacement of the MGB as well as lower pain-score were seen for the use of PRF.
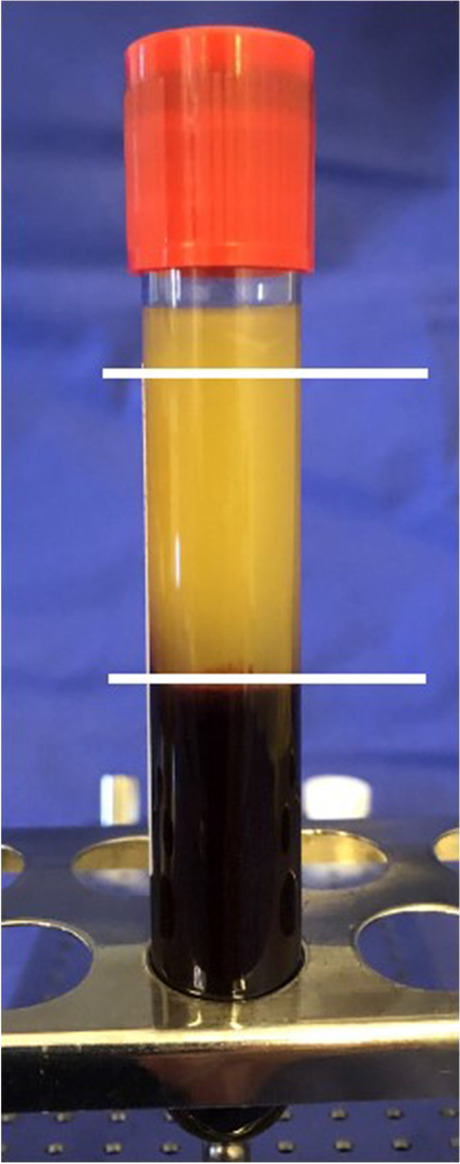
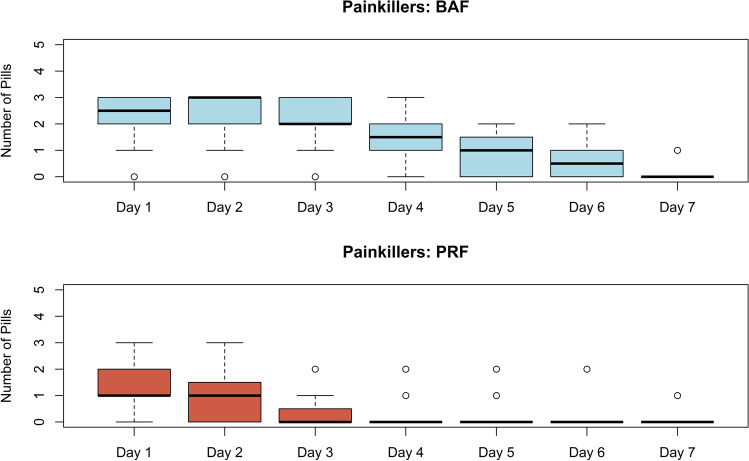
Conclusions: Based on the findings of the current study, the use of platelet-rich fibrin represents a reliable and successful method for closure of oroantral communications. The use of PRF clots for defect filling is associated with lowered pain levels and less displacement of the mucogingival border.
Clinical relevance: The defect size should be taken into account when choosing the number and size of PRF plugs.
Keywords: Buccal advancement; Closure of oroantral communications; Healing; Lukas Postl and Danilo-Marc Nadalini contributed equally to this work.; Mucogingival border; Platelet-rich fibrin.
© 2023. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Comparison of the Clinical Outcomes of Buccal Advancement Flap Versus Platelet-Rich Fibrin Application for the Immediate Closure of Acute Oroantral Communications.J Craniofac Surg. 2019 Jan;30(1):e45-e49. doi: 10.1097/SCS.0000000000004958. J Craniofac Surg. 2019. PMID: 30480627
-
The Use of Platelet-Rich Fibrin for Immediate Closure of Acute Oroantral Communications: An Alternative Approach.J Oral Maxillofac Surg. 2018 Feb;76(2):278-286. doi: 10.1016/j.joms.2017.07.168. Epub 2017 Aug 3. J Oral Maxillofac Surg. 2018. PMID: 28859924
-
The double-barrier technique using platelet-rich fibrin for closure of oroantral fistulas.J Korean Assoc Oral Maxillofac Surg. 2023 Jun 30;49(3):163-168. doi: 10.5125/jkaoms.2023.49.3.163. J Korean Assoc Oral Maxillofac Surg. 2023. PMID: 37394937 Free PMC article.
-
The effectiveness of surgical management of oroantral communications: a systematic review of the literature.Eur J Oral Implantol. 2014 Winter;7(4):347-57. Eur J Oral Implantol. 2014. PMID: 25422823 Review.
-
Is the use of platelet-rich fibrin effective in the healing, control of pain, and postoperative bleeding in the palatal area after free gingival graft harvesting? A systematic review of randomized clinical studies.Clin Oral Investig. 2021 Jul;25(7):4239-4249. doi: 10.1007/s00784-021-03933-5. Epub 2021 Apr 7. Clin Oral Investig. 2021. PMID: 33829349 Review.
Cited by
-
Treatment of Odontogenic Maxillary Sinusitis with the Use of Growth Factors in Advanced Platelet-Rich Fibrin for Immediate Closure of Oro-Antral Communication: A Case Report.Int J Mol Sci. 2024 Apr 14;25(8):4339. doi: 10.3390/ijms25084339. Int J Mol Sci. 2024. PMID: 38673924 Free PMC article.
-
Treatment of Oroantral Communication and Fistulas with the Use of Blood-Derived Platelet-Rich Preparations Rich in Growth Factors: A Systematic Review.Int J Mol Sci. 2024 Oct 26;25(21):11507. doi: 10.3390/ijms252111507. Int J Mol Sci. 2024. PMID: 39519060 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
