

Outcomes of Grade Group 2 and 3 Prostate Cancer on Initial Versus Confirmatory Biopsy: Implications for Active Surveillance
- PMID: 36566100
- PMCID: PMC10285029
- DOI: 10.1016/j.euf.2022.12.008
Outcomes of Grade Group 2 and 3 Prostate Cancer on Initial Versus Confirmatory Biopsy: Implications for Active Surveillance
Abstract
Background: Active surveillance (AS) is recommended as the preferred treatment for men with low-risk disease. In order to optimize risk stratification and exclude undiagnosed higher-grade disease, most AS protocols recommend a confirmatory biopsy.
Objective: We aimed to compare outcomes among men with grade group (GG) 2/3 prostate cancer on initial biopsy with those among men whose disease was initially GG1 but was upgraded to GG2/3 on confirmatory biopsy.
Design, setting, and participants: We reviewed patients undergoing radical prostatectomy (RP) in two cohorts: "immediate RP group," with GG2/3 cancer on diagnostic biopsy, and "AS group," with GG1 cancer on initial biopsy that was upgraded to GG2/3 on confirmatory biopsy.
Outcome measurements and statistical analysis: Probabilities of biochemical recurrence (BCR) and salvage therapy were determined using multivariable Cox regression models with risk adjustment. Risks of adverse pathology at RP were also compared using logistic regression.
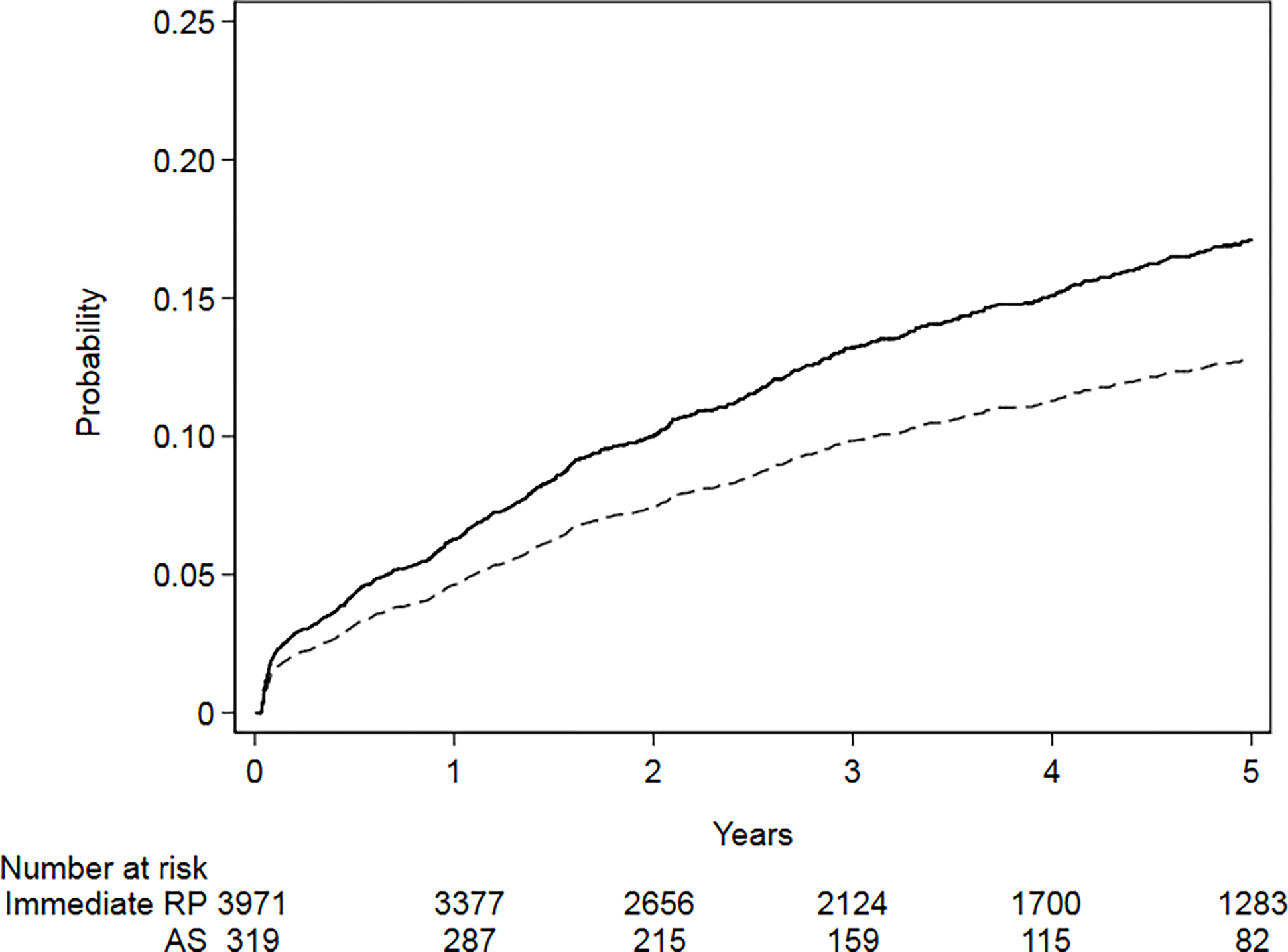
Results and limitations: The immediate RP group comprised 4009 patients and the AS group comprised 321 patients. The AS group had lower adjusted rates of adverse pathology (27% vs 35%, p = 0.003). BCR rates were lower in the AS group, although this did not reach conventional significance (hazard ratio [HR] 0.73, 95% confidence interval [CI] 0.50-1.06, p = 0.10) compared with the immediate RP group. Risk-adjusted 1- and 5-yr BCR rates were 4.6% (95% CI 3.0-6.5%) and 10.4% (95% CI 6.9-14%), respectively, for the AS group compared with 6.3% (95% CI 5.6-7.0%) and 20% (95% CI 19-22%), respectively, in the immediate RP group. A nonsignificant association was observed for salvage treatment-free survival favoring the AS group (HR 0.67, 95% CI 0.42, 1.06, p = 0.087).
Conclusions: We found that men with GG1 cancer who were upgraded on confirmatory biopsy tend to have less aggressive disease than men with the same grade found at initial biopsy. These results must be confirmed in larger series before recommendations can be made regarding a more conservative approach in men with upgraded pathology on surveillance biopsy.
Patient summary: We studied men with low-risk prostate cancer who were initially eligible for active surveillance but presented with more aggressive cancer on confirmatory biopsy. We found that outcomes for these men were better than the outcomes for those diagnosed initially with more serious cancer.
Keywords: Active surveillance; Gleason pattern; Oncological outcomes; Prognosis; Prostate cancer.
Copyright © 2022. Published by Elsevier B.V.
Conflict of interest statement
Figures

Similar articles
-
Downgrading of grade group 2 intermediate-risk prostate cancer from biopsy to radical prostatectomy: Comparison of outcomes and predictors to identify potential candidates for active surveillance.Cancer. 2020 Apr 15;126(8):1632-1639. doi: 10.1002/cncr.32709. Epub 2020 Feb 7. Cancer. 2020. PMID: 32031685
-
Effects of Initial Gleason Grade on Outcomes during Active Surveillance for Prostate Cancer.Eur Urol Oncol. 2018 Oct;1(5):386-394. doi: 10.1016/j.euo.2018.04.018. Epub 2018 May 24. Eur Urol Oncol. 2018. PMID: 31158077
-
Immediate versus delayed radical prostatectomy: updated outcomes following active surveillance of prostate cancer.Eur Urol. 2015 Sep;68(3):458-63. doi: 10.1016/j.eururo.2015.06.011. Epub 2015 Jun 29. Eur Urol. 2015. PMID: 26138041
-
Risk of Biochemical Recurrence in Patients With Grade Group 1 Prostate Cancer With Extraprostatic Extension Treated With Radical Prostatectomy.J Urol. 2024 Mar;211(3):407-414. doi: 10.1097/JU.0000000000003825. Epub 2023 Dec 18. J Urol. 2024. PMID: 38109699 Review.
-
Prostate-Specific Antigen-Based Screening for Prostate Cancer: A Systematic Evidence Review for the U.S. Preventive Services Task Force [Internet].Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 May. Report No.: 17-05229-EF-1. Rockville (MD): Agency for Healthcare Research and Quality (US); 2018 May. Report No.: 17-05229-EF-1. PMID: 30085502 Free Books & Documents. Review.
Cited by
-
Tumor upgrading among very favorable intermediate-risk prostate cancer patients treated with robot-assisted radical prostatectomy: how can it impact the clinical course?Int Urol Nephrol. 2024 Aug;56(8):2597-2605. doi: 10.1007/s11255-024-04019-3. Epub 2024 Mar 30. Int Urol Nephrol. 2024. PMID: 38553619
References
-
- Klotz L, Vesprini D, Sethukavalan P, et al. Long-term follow-up of a large active surveillance cohort of patients with prostate cancer. J Clin Oncol 2015;33:272–7. - PubMed
-
- Hamdy FC, Donovan JL, Lane JA, et al. 10-Year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med 2016;375:1415–24. - PubMed
-
- Carter G, Clover K, Britton B, et al. Wellbeing during Active Surveillance for localised prostate cancer: a systematic review of psychological morbidity and quality of life. Cancer Treat Rev 2015;41:46–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
