

Pleiomorphism plurihormonal Pit-1-positive macroadenoma with central hyperthyroidism: a rare case report and literature review
- PMID: 36539773
- PMCID: PMC9769035
- DOI: 10.1186/s12902-022-01220-2
Pleiomorphism plurihormonal Pit-1-positive macroadenoma with central hyperthyroidism: a rare case report and literature review
Abstract
Background: Thyrotropin-secreting pituitary neuroendocrine tumors (PitNETs) are rare pituitary adenomas that are occasionally accompanied by hypersecretion of other anterior pituitary hormones, such as growth hormone (GH) and prolactin (PRL). The clinical, biochemical, and pathological characteristics may represent diverse circumstances.
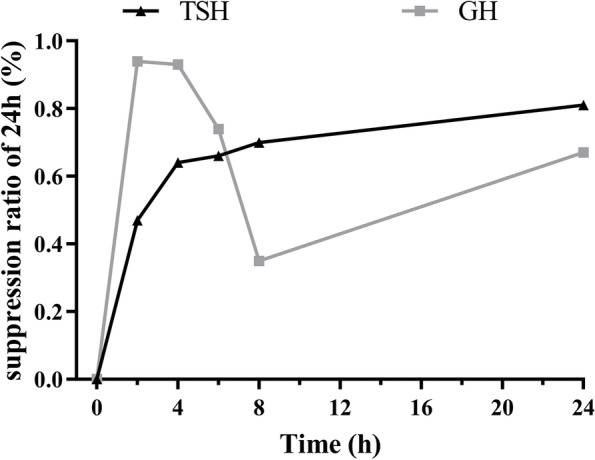
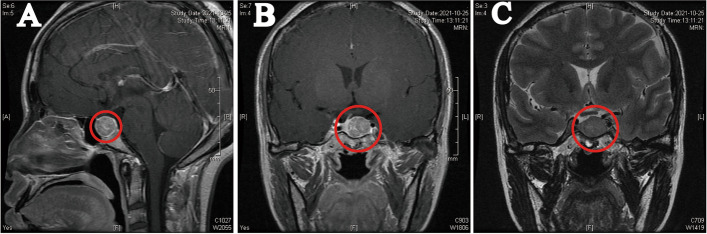
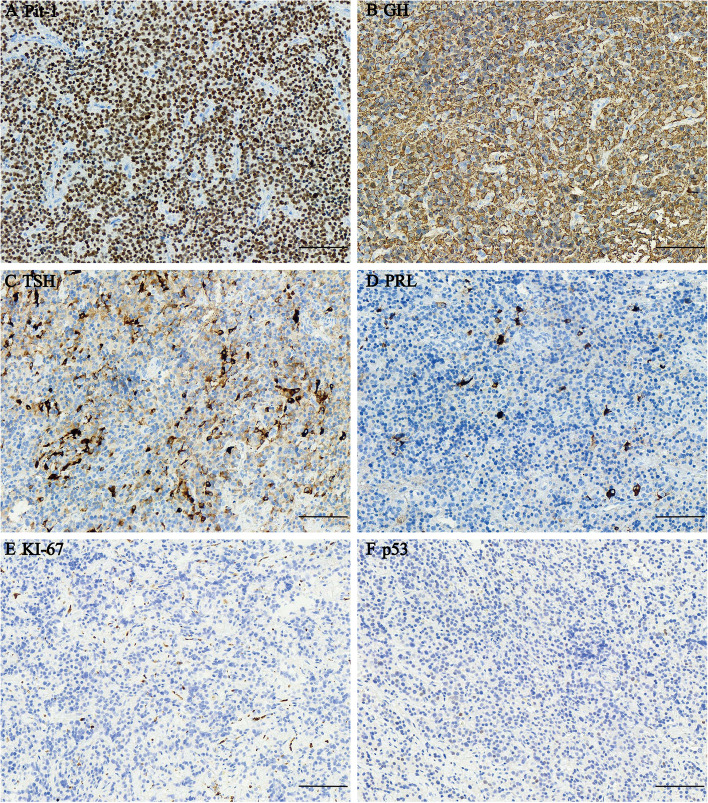
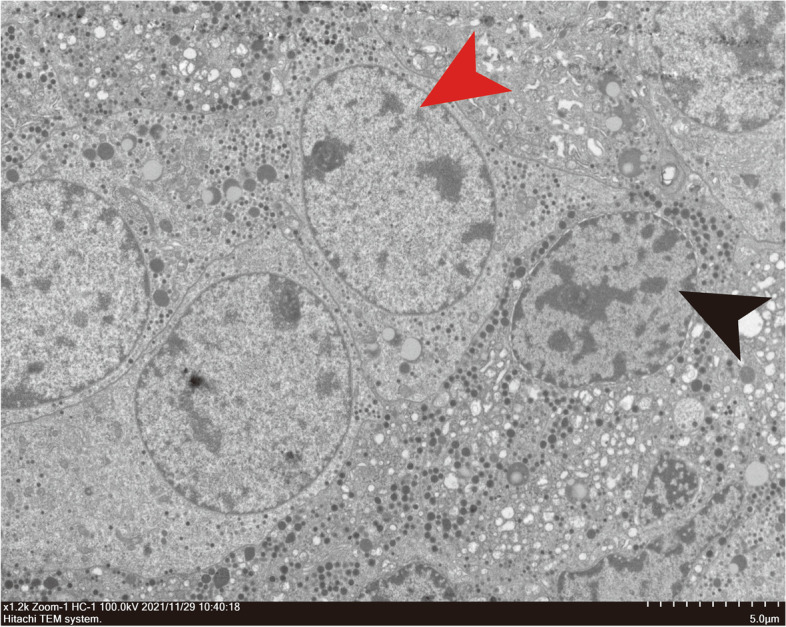
Case presentation: In this report, a 33-year-old female diagnosed with a TSH PitNET co-secreting GH presented no obvious clinical symptoms. The main characteristics were elevated thyroid-stimulating hormone (TSH), free tri-iodothyronine (FT3), and free thyroxine (FT4) levels accompanied by slightly elevated GH and insulin-like growth factor-1 (IGF-1) levels. Magnetic resonance imaging (MRI) detected a pituitary macroadenoma (18 × 16 × 16 mm) with cavernous sinus and suprasellar invasion. Immunohistochemistry revealed diffuse positivity for TSH, strong immunoreactivity for GH, and sporadic positivity for PRL. The electron microscope and double immunofluorescence staining confirmed a plurimorphous plurihormonal adenoma producing TSH, GH, and PRL. After preoperative somatostatin receptor ligand (SRL) treatment and transsphenoidal surgery, the patient achieved temporary clinical and biochemical remission. However, 3 months after surgery, the patient was suspected of having Hashimoto's thyroiditis due to higher thyroglobulin antibody (TGAb), thyroid peroxidase antibody (TPOAb), and thyroid receptor antibody (TRAb) and an enlarged thyroid nodule. During follow-up, thyroid function and TSH slowly transformed from transient hyperthyroidism to hypothyroidism. They were maintained in the normal range by L-T4.
Conclusion: In the TSH PitNET, the positive immunohistochemistry for TSH, GH, and PRL translated into hormonal overproduction with TSH and GH.
Keywords: Growth hormone (GH); Immunohistochemistry; Pituitary neuroendocrine tumor (PitNET); Plurihormonal pit-1-positive adenoma; Thyroid-stimulating hormone (TSH).
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Plurihormonal (TSH-GH-prolactin Secreting) PIT-1-Positive pituitary Macroadenoma/Pituitary Neuroendocrine Tumor (PitNET) Associated with Graves' Disease: A Case Report.Endocr Metab Immune Disord Drug Targets. 2023;23(12):1557-1561. doi: 10.2174/1871530323666230623161631. Endocr Metab Immune Disord Drug Targets. 2023. PMID: 37357515
-
Hyperthyroidism caused by an ectopic thyrotropin-secreting tumor of the nasopharynx: a case report and review of the literature.Thyroid. 2013 Sep;23(9):1172-7. doi: 10.1089/thy.2012.0574. Epub 2013 Aug 27. Thyroid. 2013. PMID: 23402621 Review.
-
Clinicopathological characteristics and therapeutic outcomes in thyrotropin-secreting pituitary adenomas: a single-center study of 90 cases.J Neurosurg. 2014 Dec;121(6):1462-73. doi: 10.3171/2014.7.JNS1471. Epub 2014 Sep 19. J Neurosurg. 2014. PMID: 25237847
-
The clinical presentation of PIT1 positive pituitary neuroendocrine tumor immunonegative for growth hormone, prolactin, and thyroid stimulating hormone with analysis of clinical and immunostaining dissociation.Clin Neurol Neurosurg. 2024 Jan;236:108075. doi: 10.1016/j.clineuro.2023.108075. Epub 2023 Nov 30. Clin Neurol Neurosurg. 2024. PMID: 38056042
-
A thyrotropin-secreting macroadenoma with positive growth hormone and prolactin immunostaining: A case report and literature review.Niger J Clin Pract. 2015 Sep-Oct;18(5):693-7. doi: 10.4103/1119-3077.158983. Niger J Clin Pract. 2015. PMID: 26096253 Review.
Cited by
-
A Case of an Immature PIT1-Lineage Pituitary Neuroendocrine Tumor of the Nasopharynx.Cureus. 2023 Sep 10;15(9):e44985. doi: 10.7759/cureus.44985. eCollection 2023 Sep. Cureus. 2023. PMID: 37701167 Free PMC article.
References
-
- Ng HY, Namboodiri D, Learoyd D, Davidson A, Champion B, Preda V. Clinical challenges of a co-secreting TSH/GH pituitary adenoma. Endocrinol Diabetes Metab Case Rep. 2019;2019:EDM190068. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
