

Hysteroscopic dilation techniques in hysteroscopic adhesiolysis
- PMID: 36481637
- PMCID: PMC10930626
- DOI: 10.11817/j.issn.1672-7347.2022.220059
Hysteroscopic dilation techniques in hysteroscopic adhesiolysis
Abstract
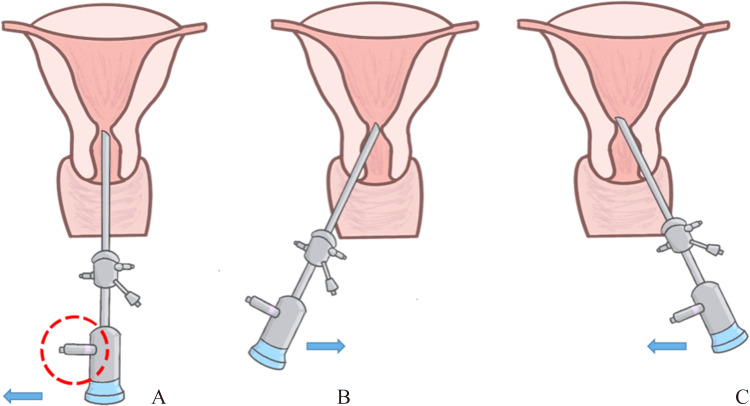
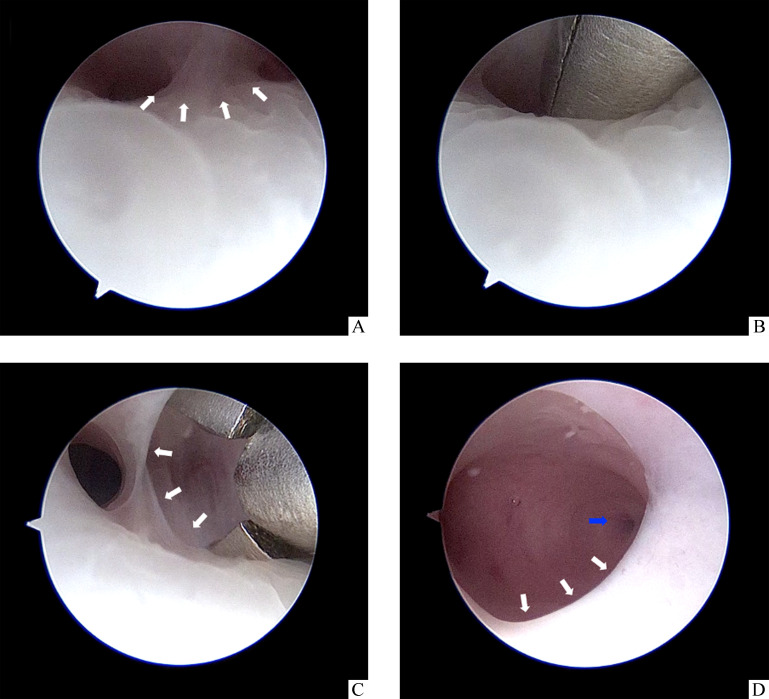
Objectives: Intrauterine adhesion (IUA) is mainly caused by intrauterine operations such as pregnancy-related curettage and hysteroscopic surgery, resulting in the trauma to the basal layer of the endometrium. Hysteroscopic adhesiolysis is a crucial step in the comprehensive treatment of IUA, and the most common complication is uterine perforation. More than half of all uterine perforations occur during the hysteroscopy or probe/dilator pass through the internal os. Furthermore, inappropriate surgical procedures may lead to endometrial injury, recurrence or even aggravation of adhesions, and complications such as cervix laceration and false passage formation. This study aims to explore the usage of the hysteroscopic dilatation techniques to dilate the internal os and lower uterine segment, which is via hysteroscopy entering the internal os laterally and swinging, or by directly opening the forceps or scissors and bluntly spreading dissection under direct hysteroscopic vision. By using the hysteroscopic dilatation techniques, we intend to improve the effectiveness and safety of cervical dilation in patients with IUA in the internal os and/or lower uterine segment.
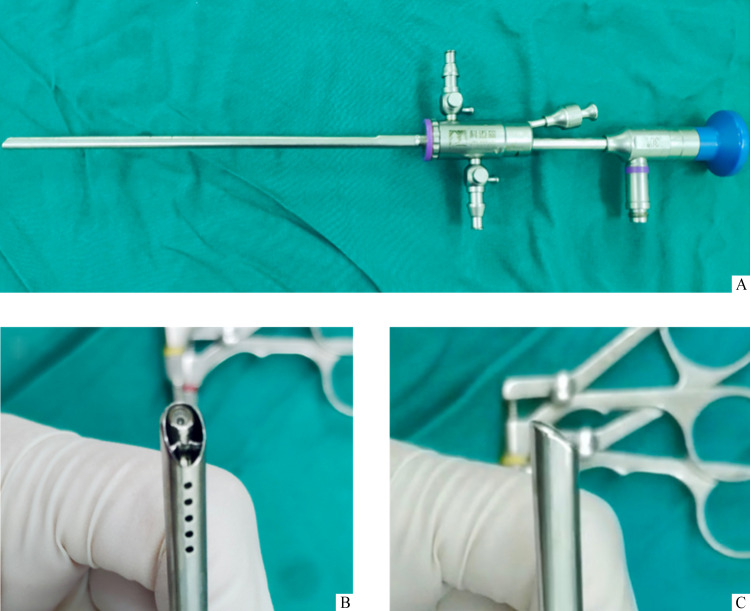
Methods: A total of 282 patients with adhesions in the internal os or lower uterine segment underwent HA in the Third Xiangya Hospital of Central South University from January 2020 to June 2021 were included, ranging from 21 to 46 (33.0±4.8) years old in age and 5 to 12 in the American Fertility Society score. Among them, there were 2 cases of false passage formation caused by traditional dilatation in other hospitals. All patients underwent hysteroscopy with integrated hysteroscopy with 5Fr instrument channel and 4.9 mm outer sheath diameter. The internal orifice of cervix and the lower segment of uterine cavity were dilated under the microscope. After the hysteroscopy entered the uterine cavity, the separation of uterine cavity adhesion and the placement of uterine contraceptive ring or uterine stent into the uterine cavity were performed routinely. Age, surgical records, and surgical videos of all included cases were collected. The success rate of dilation and the incidence of surgical complications were assessed.
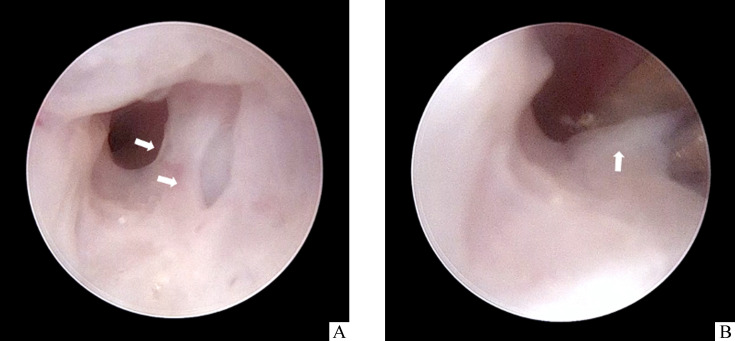
Results: In all cases, the hysteroscopys successfully entered into the uterine cavity by using the hysteroscopic dilatation techniques without failure and switching to cervical dilators. In the 2 cases of false passage due to previous cervical dilation, the uterine cavity was identified and found successfully under direct hysteroscopic vision. During the whole surgery, the vision was clear, and no complications (such as cervix laceration, false passage formation, uterine perforation or water intoxication) occurred. One to 3 months postoperative hysteroscopy revealed no significant fibrotic stenosis in the internal os and lower uterine segment.
Conclusions: The hysteroscopic dilation techniques are a strategy for separation methods that is following structural hierarchy anatomy in the mode of "see and treat" for the adhesion in the internal os and uterine cavity under direct hysteroscopic vision. This method not only has ultrasound guidance, but also has the judgment of structural hierarchy anatomy under direct hysteroscopic vision, so there is less chance of anatomical level judgment error. This method makes full use of the hysteroscopic judgement of the experienced hysteroscopic surgeons, so that surgeons can timely find and avoid re-entering the old false passage caused by previous surgery. The adhesions in the internal os and lower uterine segment were separated by the hysteroscopic dilation techniques. In this way, the damage to the endometrium caused by forced insertion of the hysteroscopy can be avoided. Meticulous separation of adhesions and cervical dilation under direct hysteroscopic vision can effectively reduce the occurrence of surgical complications such as false passage formation, cervical laceration, and uterine perforation. The use of mini-hysteroscopy eliminates the need for preoperative cervical preparation, avoiding associated risks and side effects. Moreover, for patients with adhesions in the internal os and lower uterine segment, preoperative cervical preparation is not effective in cervical dilation, while the hysteroscopic dilation techniques are effective, with higher patient acceptance due to the absence of preoperative cervical preparation. For the skilled hysteroscopic surgeons, the hysteroscopic dilation technique is easy to operate and worthy of clinical application.
目的: 宫腔粘连是一种严重影响女性生育力的疾病,多继发于妊娠相关的清宫术或宫腔镜手术等宫腔内操作,因损伤子宫内膜基底层所致。宫腔镜宫腔粘连分离术是宫腔粘连治疗环节中最关键的一步,其最常见的并发症是子宫穿孔。一半以上的子宫穿孔发生在镜体或者探针/扩宫棒通过宫颈内口阶段。在这一阶段,不恰当的手术操作还可导致内膜损伤、粘连复发加重、宫颈裂伤及假道形成等手术并发症的发生。本研究旨在提出一种宫腔镜直视下通过镜体侧入后摆动或者镜下器械直接撑开来扩张宫颈内口及宫腔下段的方法,我们称之为镜下扩宫法,以提高宫颈内口和/或宫腔下段粘连患者扩宫的有效性及安全性。方法: 收集中南大学湘雅三医院2020年1月至2021年6月行宫腔镜宫腔粘连分离术的282例患者,年龄21~46(33.0±4.8)岁,根据美国生育协会(American Fertility Society,AFS)的宫腔粘连评分标准评为5~12分,其中有2例因外院传统扩宫分离粘连所致假道形成的患者。所有患者使用具有5Fr 器械通道、4.9 mm 外鞘直径的一体式宫腔镜行宫腔镜检查。采用镜下扩宫法扩张宫颈内口及宫腔下段。宫腔镜进入宫腔后,常规行宫腔粘连分离术及向宫腔内放置宫型节育环或者宫腔支架等。收集所有纳入病例的年龄、手术记录及手术视频资料,并统计其术中镜下扩宫的成功率和手术并发症发生率。结果: 所有患者均成功利用镜下扩宫法将宫腔镜置入宫腔,2例因外院扩宫导致假道形成的患者也在镜下扩宫的过程中及时识别并成功找到宫腔。无 1例在术中因宫颈内口和宫腔下段扩张失败而中转使用传统宫颈扩张棒扩宫。整个宫腔镜手术过程中,手术视野清晰,且无假道形成、子宫穿孔或宫颈撕裂等并发症的发生。术后1至3个月复查宫腔镜,所有患者均未见宫颈内口及宫腔下段明显的粘连狭窄。结论: 镜下扩宫法是在宫腔镜直视下对粘连的宫颈内口及宫腔进行“即诊即治”模式的解剖层次分离的方法。该方法在超声引导下,通过宫腔镜直视判断解剖层次,可降低解剖层次判断错误的概率;经验丰富的宫腔镜医师能及时发现既往手术所致的陈旧性假道并避免再次进入;通过镜下分离宫颈内口及宫腔下段粘连,避免强行插入宫腔镜体而损伤内膜,可有效降低假道形成、宫颈裂伤、子宫穿孔等手术并发症的发生;采用微型宫腔镜无需术前宫颈准备,可避免相关风险和不良影响,使得术前宫颈准备扩宫效果不佳的宫颈内口及宫腔下段粘连的患者得以有效扩宫,患者接受度高。镜下扩宫法对于宫腔镜技术娴熟的术者而言操作简单,值得临床推广。.
Keywords: cervical dilation; hysteroscopic technique; infertility; intrauterine adhesions; surgical complication.
Conflict of interest statement
作者声称无任何利益冲突。
Figures

Similar articles
-
Hysteroscopic Intrauterine Adhesiolysis Using a Blunt Spreading Dissection Technique With Double-action Forceps.J Minim Invasive Gynecol. 2018 May-Jun;25(4):583-584. doi: 10.1016/j.jmig.2017.10.011. Epub 2017 Oct 13. J Minim Invasive Gynecol. 2018. PMID: 29038040
-
Clinical features of the predilection and severer sites of intrauterine adhesions.Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022 Nov 28;47(11):1568-1574. doi: 10.11817/j.issn.1672-7347.2022.220248. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022. PMID: 36481635 Free PMC article. Chinese, English.
-
Hysteroscopic Lysis of Complex Uterine Adhesions After Interventional Radiology-Guided Access.J Minim Invasive Gynecol. 2024 Jan;31(1):17-18. doi: 10.1016/j.jmig.2023.10.020. Epub 2023 Oct 31. J Minim Invasive Gynecol. 2024. PMID: 37913919
-
Hysteroscopy for treating subfertility associated with suspected major uterine cavity abnormalities.Cochrane Database Syst Rev. 2015 Feb 21;(2):CD009461. doi: 10.1002/14651858.CD009461.pub3. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2018 Dec 05;12:CD009461. doi: 10.1002/14651858.CD009461.pub4 PMID: 25701429 Updated. Review.
-
Cervical ripening before first trimester surgical evacuation for non-viable pregnancy.Cochrane Database Syst Rev. 2015 Nov 10;2015(11):CD009954. doi: 10.1002/14651858.CD009954.pub2. Cochrane Database Syst Rev. 2015. PMID: 26559875 Free PMC article. Review.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
