

Joint effects of carotid plaques and renal impairment on the risk of cardiovascular disease and all-cause death in a community-based population: The Kailuan cohort study
- PMID: 36465450
- PMCID: PMC9712795
- DOI: 10.3389/fcvm.2022.943718
Joint effects of carotid plaques and renal impairment on the risk of cardiovascular disease and all-cause death in a community-based population: The Kailuan cohort study
Abstract
Objective: It is unknown whether renal impairment and atherosclerosis increase the risk of cardiovascular disease (CVD) and death. Atherosclerosis already raises the risk of CVD and all-cause death. This study investigated the joint effects of carotid plaques and renal impairment on CVD and all-cause death in community-based populations.
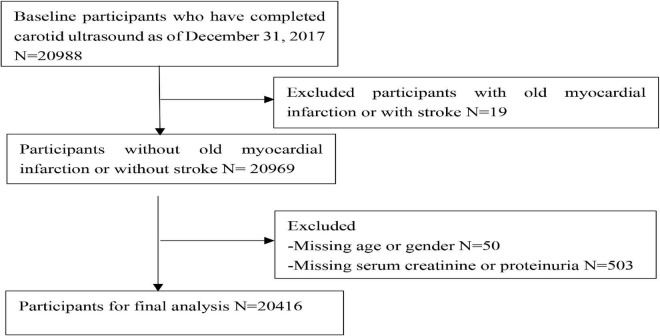
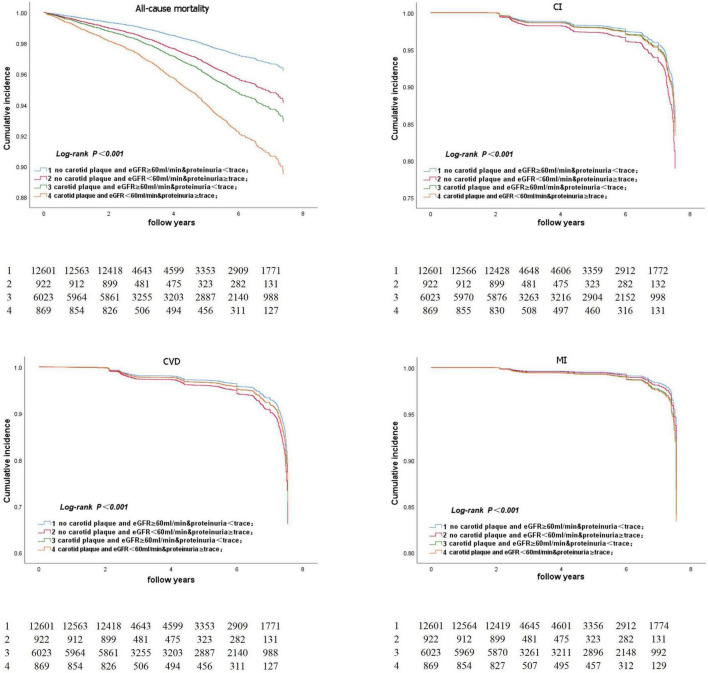
Methods: The study cohort consisted of 20,416 participants from the Kailuan Study who completed a carotid plaque ultrasound in 2012. A glomerular filtration rate (GFR) of < 60 ml/min or trace semiquantitative proteinuria or higher were both considered signs of renal insufficiency. We divided them into four groups according to the presence of carotid plaque and renal impairment. These groups were categorized as no carotid plaque, estimated glomerular filtration rate (eGFR) ≥ 60 ml/min, and proteinuria < trace; no carotid plaque, eGFR < 60 ml/min, and proteinuria ≥ trace; carotid plaque, eGFR ≥ 60 ml/min and proteinuria < trace; and carotid plaque, eGFR < 60 ml/min, and proteinuria ≥ trace, respectively. We investigated the combined effect of renal impairment and carotid plaque on cardiovascular events and all-cause death in the Kailuan community-based population.
Result: Participants with carotid plaque, eGFR < 60 ml/min and proteinuria had a 2.88-fold higher risk of all-cause death (95% CI, 2.18-3.80), which was significantly higher than those with lone factors (HR, 1.57; 95% CI, 1.04-2.36; and HR, 1.91; 95% CI, 1.56-2.32), compared to participants with no carotid plaque, eGFR ≥ 60 ml/min and proteinuria <trace group. Participants with carotid plaque, eGFR < 60 ml/min, and proteinuria had a 1.05-fold higher risk of CVD (95% CI, 0.82-1.35), which was not higher than those with alone factors (HR, 1.35; 95% CI, 1.02-1.80; and HR, 1.12; 95% CI, 0.96-1.30), compared to participants with no carotid plaque, eGFR ≥ 60 ml/min and proteinuria <trace group. Stratified analysis by age, participants with the carotid plaque, eGFR < 60 ml/min and proteinuria had a 2.98-fold higher risk of all-cause death (95% CI: 2.24-3.96), which was significantly higher than participants with lone factors (HR, 1.68; 95% CI, 1.10-2.59; and HR, 1.95; 95% CI, 1.59-2.40), compared to participants with no carotid plaque, eGFR ≥ 60 ml/min and proteinuria <trace group in the age of ≥ 50 years. Participants with carotid plaque, eGFR < 60 ml/min and proteinuria had a 1.66-fold higher risk of CVD (95% CI: 1.29-2.25), which was significantly higher than participants with lone factors (HR, 1.63; 95% CI, 1.20-2.22, and HR, 1.28; 95% CI, 1.11-1.49), compared to participants with no carotid plaque, eGFR ≥ 60 ml/min and proteinuria <trace group, in the age of ≥ 50 years.
Conclusion: The joint of carotid plaques and renal impairment may further increase the risk of CVD and all-cause death compared with participants with alone factors in the age of ≥ 50 years, but not in the age of < 50 years, from a community-based study.
Keywords: all-cause death; cardiovascular disease; carotid plaque; community-based populations; estimated glomerular filtration rate.
Copyright © 2022 Li, Bai, Miao, Chen, Zhang, Fan, Li, Wu, Liu and Hong.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer YSh declared a shared affiliation with several of the authors, WL, WB, XZ, YF, and XLi to the handling editor at the time of review.
Figures




Similar articles
-
Association of estimated glomerular filtration rate and proteinuria with all-cause mortality in community-based population in China: A Result from Kailuan Study.Sci Rep. 2018 Feb 1;8(1):2157. doi: 10.1038/s41598-018-20554-3. Sci Rep. 2018. PMID: 29391563 Free PMC article.
-
Association of Kidney Disease Measures with Cause-Specific Mortality: The Korean Heart Study.PLoS One. 2016 Apr 19;11(4):e0153429. doi: 10.1371/journal.pone.0153429. eCollection 2016. PLoS One. 2016. PMID: 27092943 Free PMC article.
-
Combined effects of carotid plaques and hypertension on the risk of cardiovascular disease and all-cause mortality.Clin Cardiol. 2020 Jul;43(7):715-722. doi: 10.1002/clc.23372. Epub 2020 May 12. Clin Cardiol. 2020. PMID: 32400055 Free PMC article.
-
Early referral strategies for management of people with markers of renal disease: a systematic review of the evidence of clinical effectiveness, cost-effectiveness and economic analysis.Health Technol Assess. 2010 Apr;14(21):1-184. doi: 10.3310/hta14210. Health Technol Assess. 2010. PMID: 20441712 Review.
-
Kidney Disease in Diabetes.In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg EW, Knowler WC, Barrett-Connor E, Becker DJ, Brancati FL, Boyko EJ, Herman WH, Howard BV, Narayan KMV, Rewers M, Fradkin JE, editors. Diabetes in America. 3rd edition. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018 Aug. CHAPTER 22. In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg EW, Knowler WC, Barrett-Connor E, Becker DJ, Brancati FL, Boyko EJ, Herman WH, Howard BV, Narayan KMV, Rewers M, Fradkin JE, editors. Diabetes in America. 3rd edition. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018 Aug. CHAPTER 22. PMID: 33651560 Free Books & Documents. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous