

Recombinant vesicular stomatitis virus-vectored vaccine induces long-lasting immunity against Nipah virus disease
- PMID: 36445779
- PMCID: PMC9888376
- DOI: 10.1172/JCI164946
Recombinant vesicular stomatitis virus-vectored vaccine induces long-lasting immunity against Nipah virus disease
Abstract
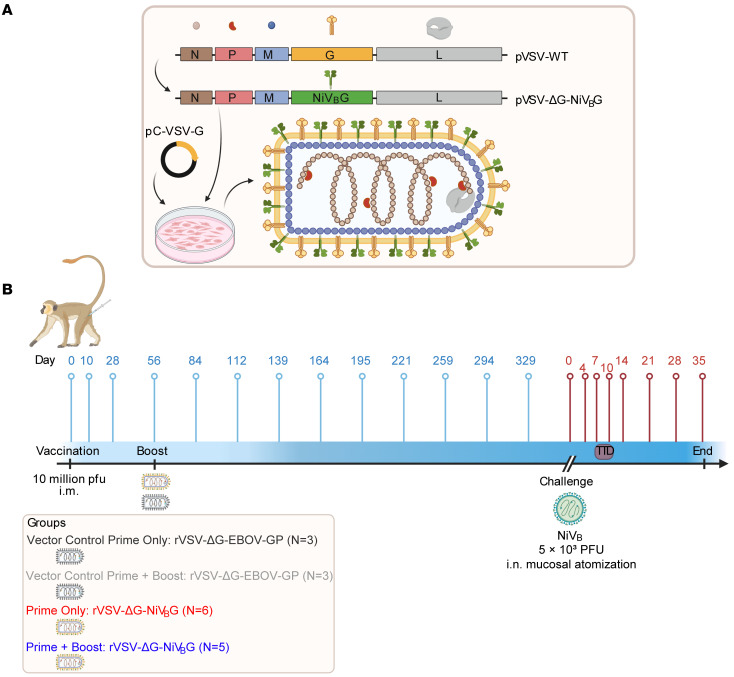
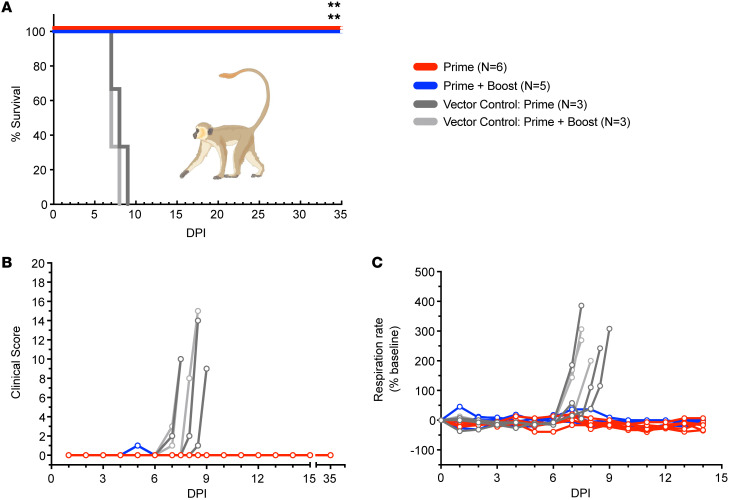
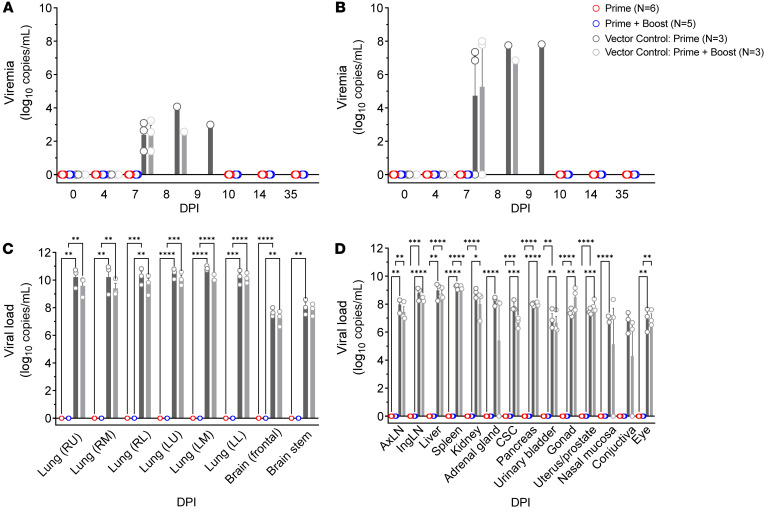
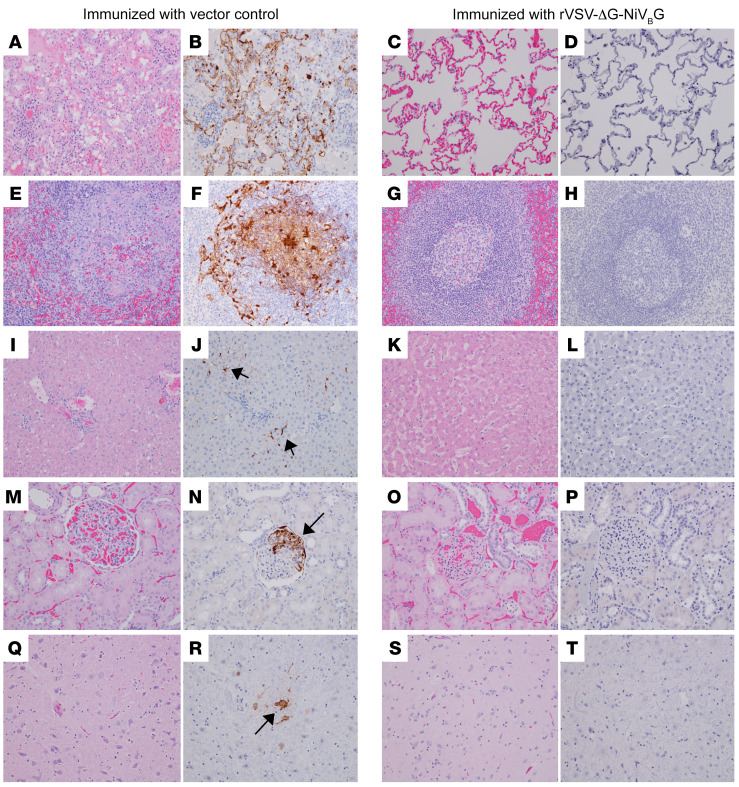
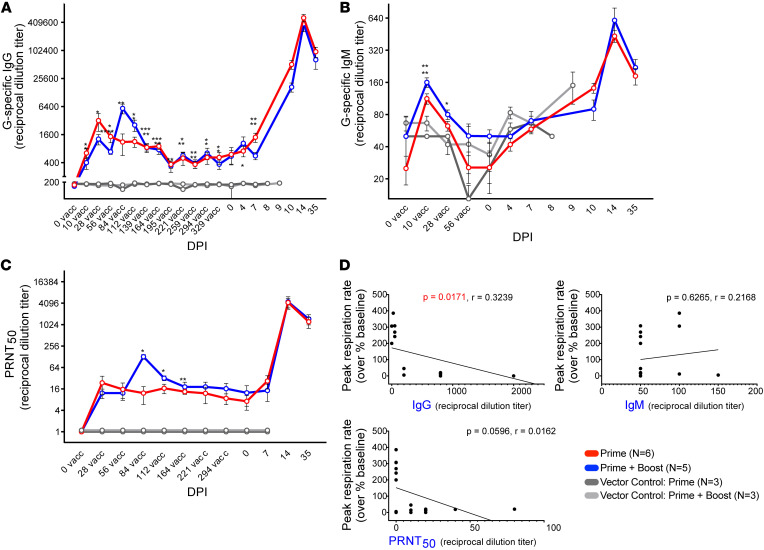
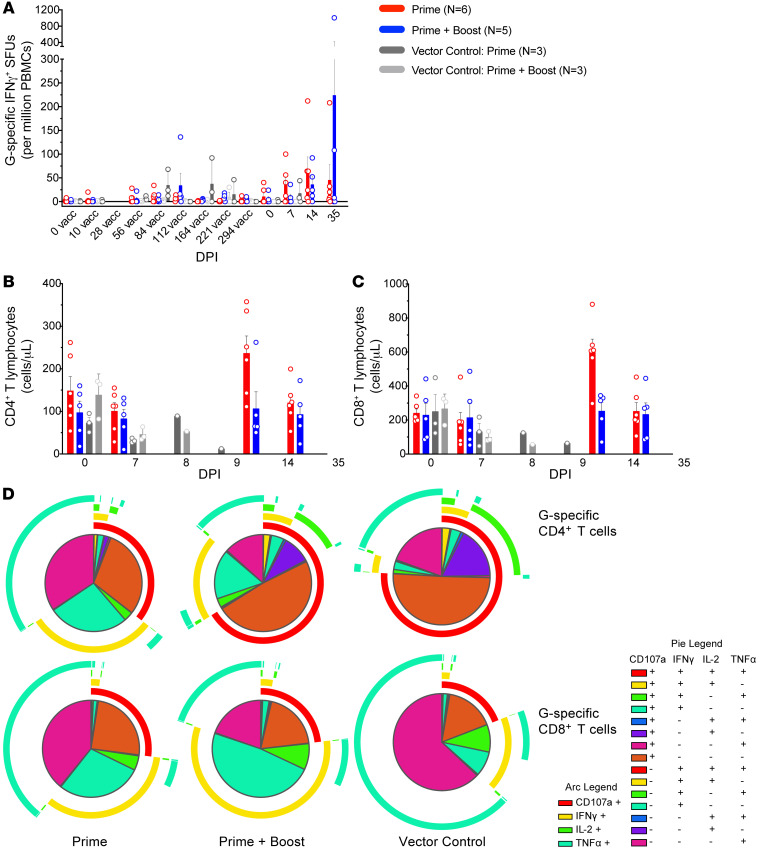
The emergence of the novel henipavirus, Langya virus, received global attention after the virus sickened over three dozen people in China. There is heightened concern that henipaviruses, as respiratory pathogens, could spark another pandemic, most notably the deadly Nipah virus (NiV). NiV causes near-annual outbreaks in Bangladesh and India and induces a highly fatal respiratory disease and encephalitis in humans. No licensed countermeasures against this pathogen exist. An ideal NiV vaccine would confer both fast-acting and long-lived protection. Recently, we reported the generation of a recombinant vesicular stomatitis virus-based (rVSV-based) vaccine expressing the NiV glycoprotein (rVSV-ΔG-NiVBG) that protected 100% of nonhuman primates from NiV-associated lethality within a week. Here, to evaluate the durability of rVSV-ΔG-NiVBG, we vaccinated African green monkeys (AGMs) one year before challenge with an uniformly lethal dose of NiV. The rVSV-ΔG-NiVBG vaccine induced stable and robust humoral responses, whereas cellular responses were modest. All immunized AGMs (whether receiving a single dose or prime-boosted) survived with no detectable clinical signs or NiV replication. Transcriptomic analyses indicated that adaptive immune signatures correlated with vaccine-mediated protection. While vaccines for certain respiratory infections (e.g., COVID-19) have yet to provide durable protection, our results suggest that rVSV-ΔG-NiVBG elicits long-lasting immunity.
Keywords: Adaptive immunity; Infectious disease; Vaccines.
Conflict of interest statement
Figures
Similar articles
-
Single-dose live-attenuated Nipah virus vaccines confer complete protection by eliciting antibodies directed against surface glycoproteins.Vaccine. 2014 May 7;32(22):2637-44. doi: 10.1016/j.vaccine.2014.02.087. Epub 2014 Mar 12. Vaccine. 2014. PMID: 24631094 Free PMC article.
-
Immunological correlates of protection afforded by PHV02 live, attenuated recombinant vesicular stomatitis virus vector vaccine against Nipah virus disease.Front Immunol. 2023 Sep 4;14:1216225. doi: 10.3389/fimmu.2023.1216225. eCollection 2023. Front Immunol. 2023. PMID: 37731485 Free PMC article.
-
Use of Single-Injection Recombinant Vesicular Stomatitis Virus Vaccine to Protect Nonhuman Primates Against Lethal Nipah Virus Disease.Emerg Infect Dis. 2019 Jun;25(6):1144-1152. doi: 10.3201/eid2506.181620. Emerg Infect Dis. 2019. PMID: 31107231 Free PMC article.
-
Recombinant vesicular stomatitis virus-based vaccines against Ebola and Marburg virus infections.J Infect Dis. 2011 Nov;204 Suppl 3(Suppl 3):S1075-81. doi: 10.1093/infdis/jir349. J Infect Dis. 2011. PMID: 21987744 Free PMC article. Review.
-
Advancements in Nipah virus treatment: Analysis of current progress in vaccines, antivirals, and therapeutics.Immunology. 2024 Feb;171(2):155-169. doi: 10.1111/imm.13695. Epub 2023 Sep 15. Immunology. 2024. PMID: 37712243 Review.
Cited by
-
Animal Models for Henipavirus Research.Viruses. 2023 Sep 22;15(10):1980. doi: 10.3390/v15101980. Viruses. 2023. PMID: 37896758 Free PMC article. Review.
-
A potent Henipavirus cross-neutralizing antibody reveals a dynamic fusion-triggering pattern of the G-tetramer.Nat Commun. 2024 May 21;15(1):4330. doi: 10.1038/s41467-024-48601-w. Nat Commun. 2024. PMID: 38773072 Free PMC article.
-
A vaccine targeting antigen-presenting cells through CD40 induces protective immunity against Nipah disease.Cell Rep Med. 2024 Mar 19;5(3):101467. doi: 10.1016/j.xcrm.2024.101467. Epub 2024 Mar 11. Cell Rep Med. 2024. PMID: 38471503 Free PMC article.
-
A systematic review on Nipah virus: global molecular epidemiology and medical countermeasures development.Virus Evol. 2024 Jul 25;10(1):veae048. doi: 10.1093/ve/veae048. eCollection 2024. Virus Evol. 2024. PMID: 39119137 Free PMC article.
-
Prospects and Challenges in Developing mRNA Vaccines for Infectious Diseases and Oncogenic Viruses.Med Sci (Basel). 2024 May 22;12(2):28. doi: 10.3390/medsci12020028. Med Sci (Basel). 2024. PMID: 38804384 Free PMC article. Review.
References
-
- WHO. Fact Sheets: Nipah Virus. https://www.who.int/news-room/fact-sheets/detail/nipah-virus Updated May 30, 2018. Accessed November 23, 2022.
-
- Federal Register. Possession, Use, and Transfer of Select Agents and Toxins; Biennial Review (HHS/CDC): Select Agents and Toxins, 42 CFR Part 73. Volume 85, No. 52, p. 15087. https://www.govinfo.gov/content/pkg/FR-2020-03-17/pdf/2020-05477.pdf Updated March 17, 2020. Accessed November 23, 2022.
-
- CDC/US Department of Agriculture. Federal Select Agent Program: HHS and USDA Select Agents and Toxins, 7 CFR Part 331, 9 CFR Part 121, and 42 CFR Part 73. https://www.selectagents.gov/sat/list.htm?CDC_AA_refVal=https%3A%2F%2Fww... Updated August 30, 2022. Accessed November 23, 2022.
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
