

Predictive value of neutrophil-to-lymphocyte and platelet ratio in in-hospital mortality in septic patients
- PMID: 36439769
- PMCID: PMC9681647
- DOI: 10.1016/j.heliyon.2022.e11498
Predictive value of neutrophil-to-lymphocyte and platelet ratio in in-hospital mortality in septic patients
Abstract
Background: Among critically ill patients in the intensive care unit (ICU), sepsis is an urgent global public health problem due to its high incidence, high mortality rate and complex pathogenesis.
Objective: This study was to evaluate the predictive value of neutrophil-to-lymphocyte ratio (NLR), and neutrophil-to-lymphocyte and platelet ratio (NLPR) in-hospital mortality in septic patients on days 1, 3 and 5 in ICU.
Methods: The data of septic patients admitted to the ICU of the Sixth Affiliated Hospital of Sun Yat-sen University from March, 2018 to July, 2019 were collected. NLR and NLPR were calculated and multivariate logistic regression analysis was performed to identify the relationship between them and in-hospital mortality, respectively. Receiver operating characteristic curve (ROC) was used to determine the efficacy and optimal cutoff value of diagnostic tests.
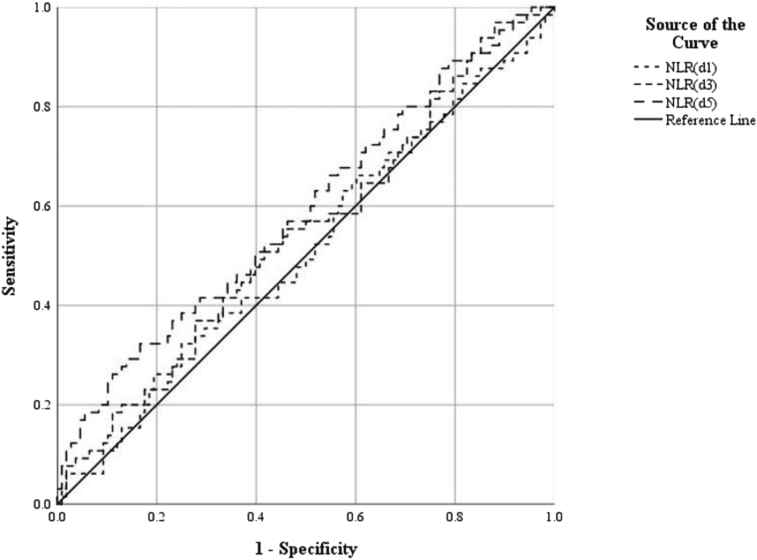
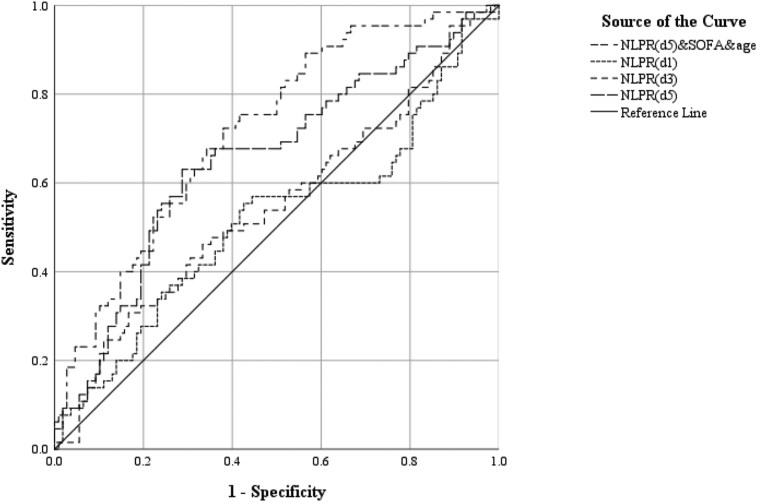
Results: A total of 173 septic patients were included in this analysis, including 108 cases in the survival group and 65 in the death group, with a total mortality rate of 37.6%. A multivariate logistic regression analysis showed that NLR on day 5 was independently correlated with in-hospital mortality rate (OR 1.041, 95% CI: 1.008-1.074), and Day 5 NLPR was also independently associated with in-hospital mortality rate (OR 1.020, 95% CI: 1.001-1.040). The areas under the receiver operating characteristic curve (AUC) of the NLR on days 1 and 3 was 0.513 and 0.542 respectively, and the optimal cutoff value were 23.16 and 15.48, and the AUC of the NLR on day 5 was 0.589, and the best cutoff value was 15.85. The AUC of NLPR on day 1 and 3 was 0.517 and 0.547, respectively, and the optimal cutoff value was 10.25 and 18.47. The AUC of NLPR on day 5 was the largest, 0.654, and the optimal cutoff value was 8.22. After combined NLPR on day 5 with age and sequential organ failure assessment (SOFA) scores, the AUC increase to 0.718. Among the joint predictors, the optimal cutoff value for NLPR on day 5 was 9.31.
Conclusion: We found that Day 5 NLPR and NLR were independently correlated with in-hospital mortality. Day 5 NLPR Combined with age and SOFA scores may be help predict mortality in ICU septic hospitalized patients.
Keywords: Lymphocyte; Mortality; Neutrophil; Platelet; Sepsis.
© 2022 The Author(s).
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
The systemic inflammation indexes after admission predict in-hospital mortality in patients with extensive burns.Burns. 2024 May;50(4):980-990. doi: 10.1016/j.burns.2024.01.020. Epub 2024 Jan 20. Burns. 2024. PMID: 38336497
-
[Combined prognostic value of serum lactic acid, procalcitonin and severity score for short-term prognosis of septic shock patients].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021 Mar;33(3):281-285. doi: 10.3760/cma.j.cn121430-20201113-00715. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2021. PMID: 33834968 Chinese.
-
Immune cell composition and its impact on prognosis in children with sepsis.BMC Pediatr. 2024 Sep 28;24(1):611. doi: 10.1186/s12887-024-05087-1. BMC Pediatr. 2024. PMID: 39342149 Free PMC article.
-
Urinary neutrophil gelatinase-associated lipocalin was a predictor from the day after intensive care unit entry, but not on the day of intensive care unit entry.Clin Chim Acta. 2021 Jun;517:117-121. doi: 10.1016/j.cca.2021.02.017. Epub 2021 Mar 2. Clin Chim Acta. 2021. PMID: 33667482
-
The prognostic value of the combined neutrophil-to-lymphocyte ratio (NLR) and neutrophil-to-platelet ratio (NPR) in sepsis.Sci Rep. 2024 Jul 2;14(1):15075. doi: 10.1038/s41598-024-64469-8. Sci Rep. 2024. PMID: 38956445 Free PMC article.
Cited by
-
Predictive Value of Neutrophil-Lymphocyte Ratio and Other Inflammation Indices in Febrile Seizures in Children.J Clin Med. 2024 Sep 9;13(17):5330. doi: 10.3390/jcm13175330. J Clin Med. 2024. PMID: 39274543 Free PMC article.
-
Neutrophil-to-lymphocyte ratio, monocyte-to-lymphocyte ratio, platelet-to-lymphocyte ratio associated with 28-day all-cause mortality in septic patients with coronary artery disease: a retrospective analysis of MIMIC-IV database.BMC Infect Dis. 2024 Jul 29;24(1):749. doi: 10.1186/s12879-024-09516-5. BMC Infect Dis. 2024. PMID: 39075364 Free PMC article.
-
U-shaped correlation of lymphocyte count with all-cause hospital mortality in sepsis and septic shock patients: a MIMIC-IV and eICU-CRD database study.Int J Emerg Med. 2024 Aug 26;17(1):101. doi: 10.1186/s12245-024-00682-6. Int J Emerg Med. 2024. PMID: 39187746 Free PMC article.
-
Nutritional State, Immunological and Biochemical Parameters, and Mortality in the ICU: An Analytical Study.J Clin Med. 2023 Jun 21;12(13):4177. doi: 10.3390/jcm12134177. J Clin Med. 2023. PMID: 37445212 Free PMC article.
-
Diagnostic accuracy of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, and neutrophil-lymphocyte-to-platelet ratio biomarkers in predicting bacteremia and sepsis in immunosuppressive patients with cancer: literature review.Porto Biomed J. 2024 Jun 4;9(3):254. doi: 10.1097/j.pbj.0000000000000254. eCollection 2024 May-Jun. Porto Biomed J. 2024. PMID: 38835655 Free PMC article. Review.
References
-
- Gaborit B.J., Chaumette T., Chauveau M., Asquier-Khati A., Roquilly A., Boutoille D., et al. Circulating regulatory T cells expressing tumor necrosis factor receptor type 2 contribute to sepsis-induced immunosuppression in patients during septic shock. J. Infect. Dis. 2021;224(12):2160–2169. - PubMed
-
- Burke J., Wood S., Hermon A., Szakmany T. Improving outcome of sepsis on the ward: introducing the 'Sepsis Six' bundle. Nurs. Crit. Care. 2019;24(1):33–39. - PubMed
-
- Fleischmann C., Scherag A., Adhikari N.K., Hartog C.S., Tsaganos T., Schlattmann P., et al. Assessment of global incidence and mortality of hospital-treated sepsis. Current estimates and limitations. Am. J. Respir. Crit. Care Med. 2016;193(3):259–272. - PubMed
LinkOut - more resources
Full Text Sources
