

Out-of-hospital health care costs of childhood food allergy in Australia: A population-based longitudinal study
- PMID: 36433856
- PMCID: PMC9828422
- DOI: 10.1111/pai.13883
Out-of-hospital health care costs of childhood food allergy in Australia: A population-based longitudinal study
Abstract
Background: Australia has one of the highest prevalence of childhood food allergy in the world, but there are no data on its economic burden in Australia.
Methods: We used data from the HealthNuts study, a population-based longitudinal study undertaken in Melbourne, Australia. Infants were recruited at age 12 months between Sept 2007 and Aug 2011 with food allergy diagnosed using oral food challenges. Health care costs of out-of-hospital services were collected through data linkage to Australia's universal health insurance scheme Medicare. Two-part model was used to compare costs after controlling for potential confounders.
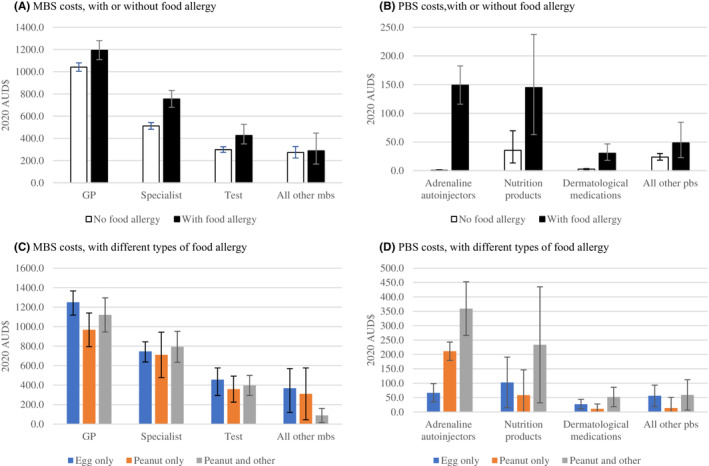
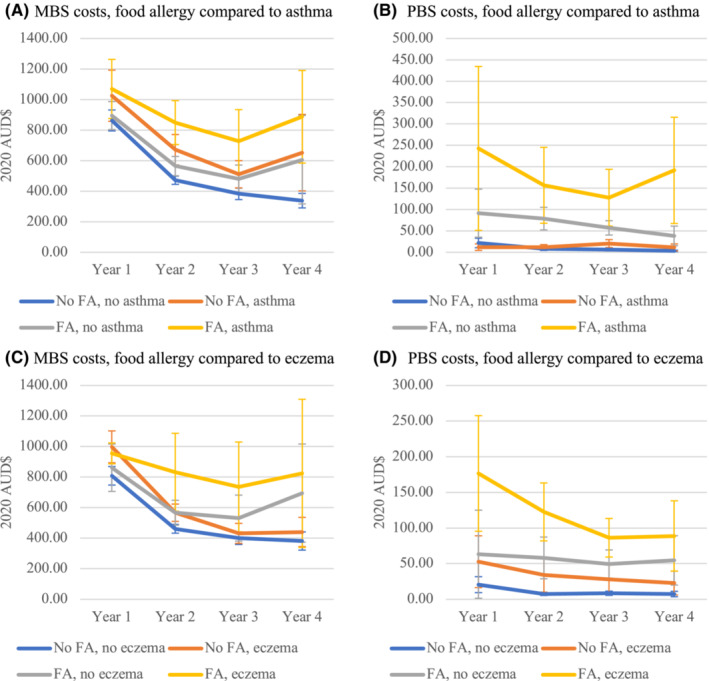
Results: 2919 children were included, and 390 (13.4%) had challenge-confirmed food allergy at age 1 year. Compared with children without food allergy, children with food allergy had significantly higher costs for GP visits, specialist visits, tests, and prescriptions in the first four years of life. The total Medicare cost associated with food allergy from age 1 to 4 years was estimated to be AUD$889.7 (95% CI $566.1-$1188.3) or €411.0 (95% CI €261.5-€549.0) per child. This was projected into an annual Medicare cost of AUD$26.1 million (95% CI $20.1-$32.3 million) or €12.1 (95% CI €9.3-€14.9 million) based on population size in 2020.
Conclusions: Childhood food allergy causes considerable Medicare costs for out-of-hospital services in the first four years after birth in Australia. These findings can help anticipate the financial impact on the health care system associated with childhood food allergy, act as a useful costing resource for future evaluations, and inform management of childhood food allergy internationally.
Keywords: burden; child; food allergy; health care costs.
© 2022 The Authors. Pediatric Allergy and Immunology published by European Academy of Allergy and Clinical Immunology and John Wiley & Sons Ltd.
Conflict of interest statement
Kirsten Perrett is Chair of the scientific advisory board for AllergyPal. Her institution has received research grants from the National Health and Medical Research Council, Immune Tolerance Network, DBV Technologies, and Novartis and consultant fees from Aravax; outside the submitted work. Other authors declare no conflict of interest. S.C.D. and A.J.L. declare they have received research funds from GSK’s competitively awarded Investigator Sponsored Studies programme, for unrelated research. A.J.L. has also received donations of interventional product (EpiCeram) from Primus Pharmaceuticals for unrelated research.
Figures
Similar articles
-
The prevalence of food allergy and other allergic diseases in early childhood in a population-based study: HealthNuts age 4-year follow-up.J Allergy Clin Immunol. 2017 Jul;140(1):145-153.e8. doi: 10.1016/j.jaci.2017.02.019. Epub 2017 May 14. J Allergy Clin Immunol. 2017. PMID: 28514997
-
Costs and uptake of a community model of paediatric food allergy care versus specialist hospital care: A before-and-after controlled trial.J Paediatr Child Health. 2020 Aug;56(8):1225-1232. doi: 10.1111/jpc.14905. Epub 2020 May 15. J Paediatr Child Health. 2020. PMID: 32412683 Clinical Trial.
-
Primary health-care costs associated with special health care needs up to age 7 years: Australian population-based study.J Paediatr Child Health. 2014 Oct;50(10):768-74. doi: 10.1111/jpc.12649. Epub 2014 Jun 13. J Paediatr Child Health. 2014. PMID: 24923806
-
Epidemiology of childhood food allergy.Pediatr Ann. 2013 Jun 1;42(6):91-5. doi: 10.3928/00904481-20130522-08. Pediatr Ann. 2013. PMID: 23718236 Review.
-
Clinical spectrum of food allergy in children in Australia and South-East Asia: identification and targets for treatment.Ann Med. 1999 Aug;31(4):272-81. doi: 10.3109/07853899908995890. Ann Med. 1999. PMID: 10480758 Review.
Cited by
-
The Natural History and Risk Factors for the Development of Food Allergies in Children and Adults.Curr Allergy Asthma Rep. 2024 Mar;24(3):121-131. doi: 10.1007/s11882-024-01131-3. Epub 2024 Feb 28. Curr Allergy Asthma Rep. 2024. PMID: 38416390 Free PMC article. Review.
References
-
- Osborne NJ, Koplin JJ, Martin PE, et al. Prevalence of challenge‐proven IgE‐mediated food allergy using population‐based sampling and predetermined challenge criteria in infants. J Allergy Clin Immunol. 2011;127(3):668‐676.e2. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
