

Crohn's disease patients with L4-esophagogastroduodenal phenotype is associated with a better prognosis: A retrospective cohort study
- PMID: 36386193
- PMCID: PMC9649486
- DOI: 10.3389/fphar.2022.963892
Crohn's disease patients with L4-esophagogastroduodenal phenotype is associated with a better prognosis: A retrospective cohort study
Abstract
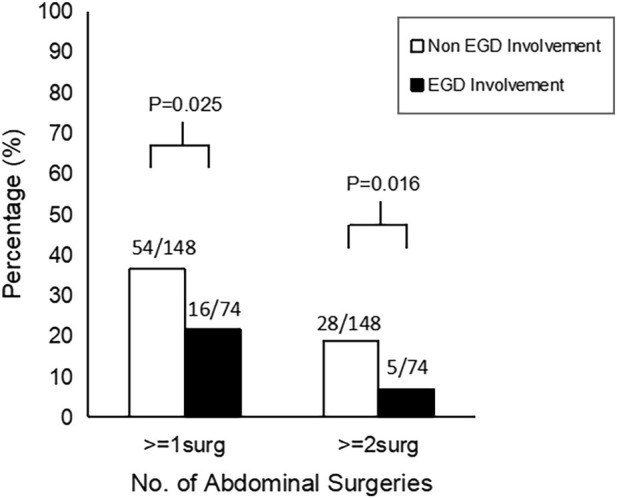
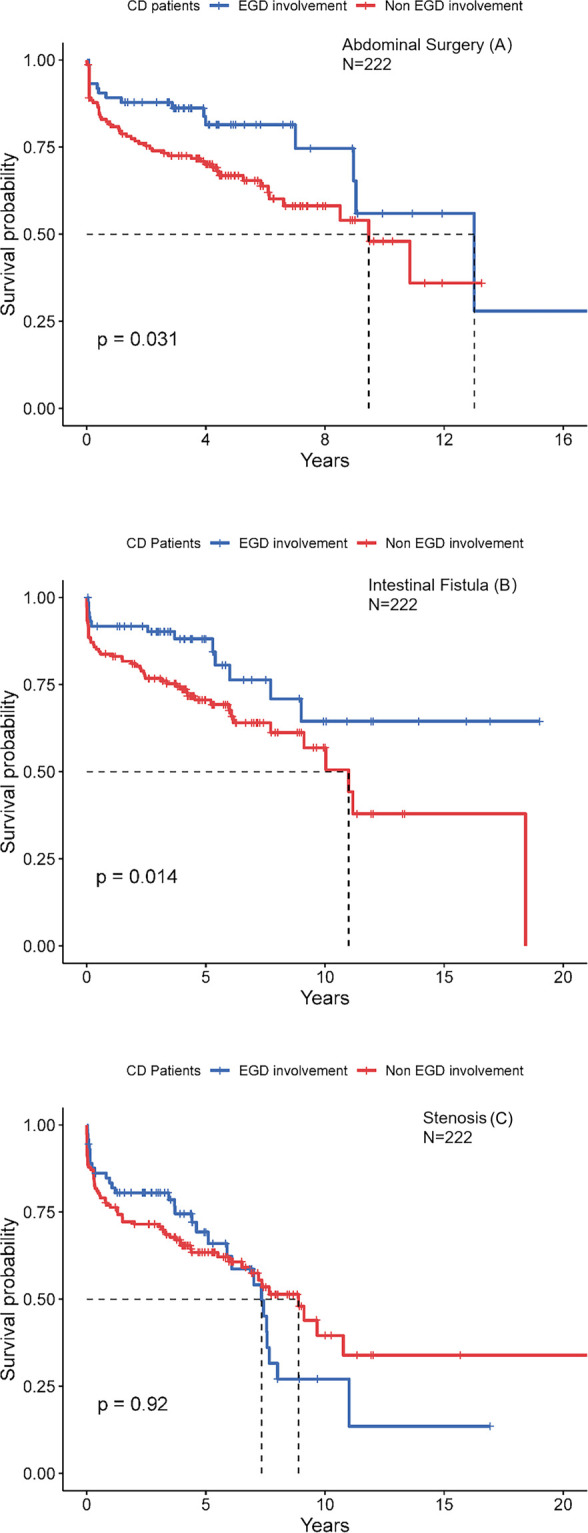
Background: In the Montreal classification, L4 Crohn's disease (CD) is defined as an ileal disease, including L4-esophagogastric duodenum (EGD), L4-jejunum, and L4-proximal ileal involvement. According to the previous studies, the prognosis of L4 disease was worse than that of non-L4 disease. Among L4 diseases, the phenotypes of L4-jejunum and L4-proximal ileum indicated that the risk of abdominal surgery was higher. However, the prognosis of L4-esophagogastroduodenal remains largely elusive. Therefore, we aim to investigate whether the prognosis differs between CD patients with and without esophagogastroduodenal involvement. Methods: In this study, patients with L4-EGD phenotype (n = 74) who underwent gastroscopy, ileocolonoscopy, biopsies, and CTE from 2018 to 2020 were compared with L4 non-EGD controls (n = 148) who were randomly selected at a ratio of 1:2 in the same period. Demographic information inclusive of disease conduct and location, important points of the surgery, and hospitalization have been collected. The distinction between L4-EGD patients and non-L4-EGD patients was identified by way of multivariable logistic regression analysis. The Kaplan-Meier technique was used to consider the possibility of abdominal surgical operation and complications, observed by means of Cox percentage hazard fashions to decide if L4 EGD independently estimated the endpoints inclusive of the abdominal surgery and the occurrences of complications. Results: L4-EGD group (n = 74) had a lower proportion of intestinal fistula than the control group (n = 148) (17.6% versus 34.5%; p = 0.009), and the probabilities of requiring abdominal surgery and multiple abdominal surgeries were also lower (21.6% versus 36.5%; p = 0.025), (6.8% versus 18.9%; p = 0.016), respectively. The frequency of hospitalization was lower in the L4-EGD group than in the control group (3-7 versus 4-9; p = 0.013). L4-EGD phenotype was found to be an independent protective factor for abdominal surgery and intestinal fistula in the Cox regression model, with HRs of 0.536 (95%CI: 0.305-0.940; p = 0.030) and 0.478 (95%CI: 0.259-0.881; p = 0.018), respectively. Conclusion: Our data suggest that the L4-EGD phenotype may have a better prognosis compared to the Non-L4-EGD phenotype. Our data may advocate a revision of the Montreal classification including separate designations for L4-EGD disease.
Keywords: Abdominal surgery; Complication; Crohn’s disease; EGD involvement; Prognosis.
Copyright © 2022 Weng, Lin, Chen, Liang, Xu, Cai, Lu, Rong, Zou and Zhu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Different clinical outcomes in Crohn's disease patients with esophagogastroduodenal, jejunal, and proximal ileal disease involvement: is L4 truly a single phenotype?Therap Adv Gastroenterol. 2018 Jun 5;11:1756284818777938. doi: 10.1177/1756284818777938. eCollection 2018. Therap Adv Gastroenterol. 2018. PMID: 29899757 Free PMC article.
-
Relationship between proximal Crohn's disease location and disease behavior and surgery: a cross-sectional study of the IBD Genetics Consortium.Am J Gastroenterol. 2013 Jan;108(1):106-12. doi: 10.1038/ajg.2012.389. Epub 2012 Dec 11. Am J Gastroenterol. 2013. PMID: 23229423 Free PMC article.
-
Clinical Features and Prognosis of Crohn's Disease with Upper Gastrointestinal Tract Phenotype in Chinese Patients.Dig Dis Sci. 2019 Nov;64(11):3291-3299. doi: 10.1007/s10620-019-05651-1. Epub 2019 May 11. Dig Dis Sci. 2019. PMID: 31079261
-
Visceral adiposity and inflammatory bowel disease.Int J Colorectal Dis. 2021 Nov;36(11):2305-2319. doi: 10.1007/s00384-021-03968-w. Epub 2021 Jun 9. Int J Colorectal Dis. 2021. PMID: 34104989 Review.
-
Upper gastrointestinal tract phenotype of Crohn's disease is associated with early surgery and further hospitalization.Inflamm Bowel Dis. 2009 Apr;15(4):551-7. doi: 10.1002/ibd.20804. Inflamm Bowel Dis. 2009. PMID: 19067420
Cited by
-
Are We Ready to Reclassify Crohn's Disease Using Molecular Classification?J Clin Med. 2023 Sep 5;12(18):5786. doi: 10.3390/jcm12185786. J Clin Med. 2023. PMID: 37762727 Free PMC article.
-
Upper Gastrointestinal Involvement in Crohn's Disease as an Independent Predictor of New-Onset Strictures: Insights from an Extensive Retrospective Cohort Analysis.Dig Dis Sci. 2024 Sep;69(9):3382-3391. doi: 10.1007/s10620-024-08577-5. Epub 2024 Aug 1. Dig Dis Sci. 2024. PMID: 39090445
References
LinkOut - more resources
Full Text Sources