

Human type I IFN deficiency does not impair B cell response to SARS-CoV-2 mRNA vaccination
- PMID: 36342455
- PMCID: PMC9814155
- DOI: 10.1084/jem.20220258
Human type I IFN deficiency does not impair B cell response to SARS-CoV-2 mRNA vaccination
Abstract
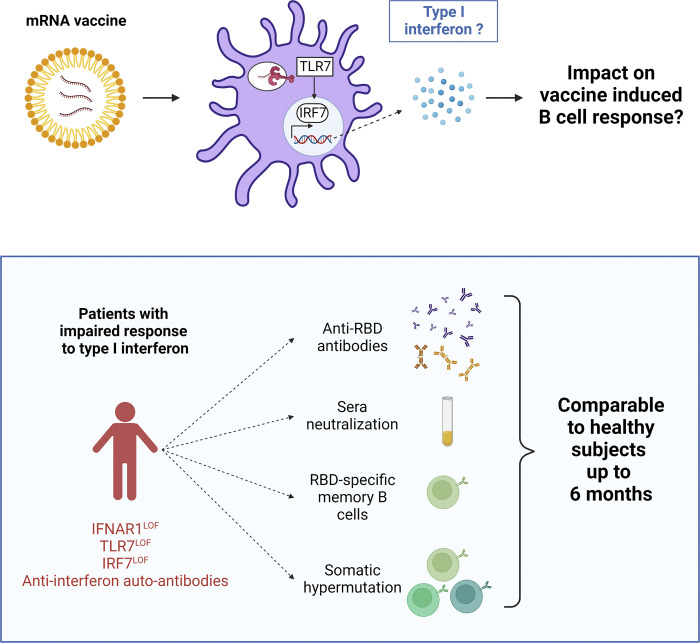
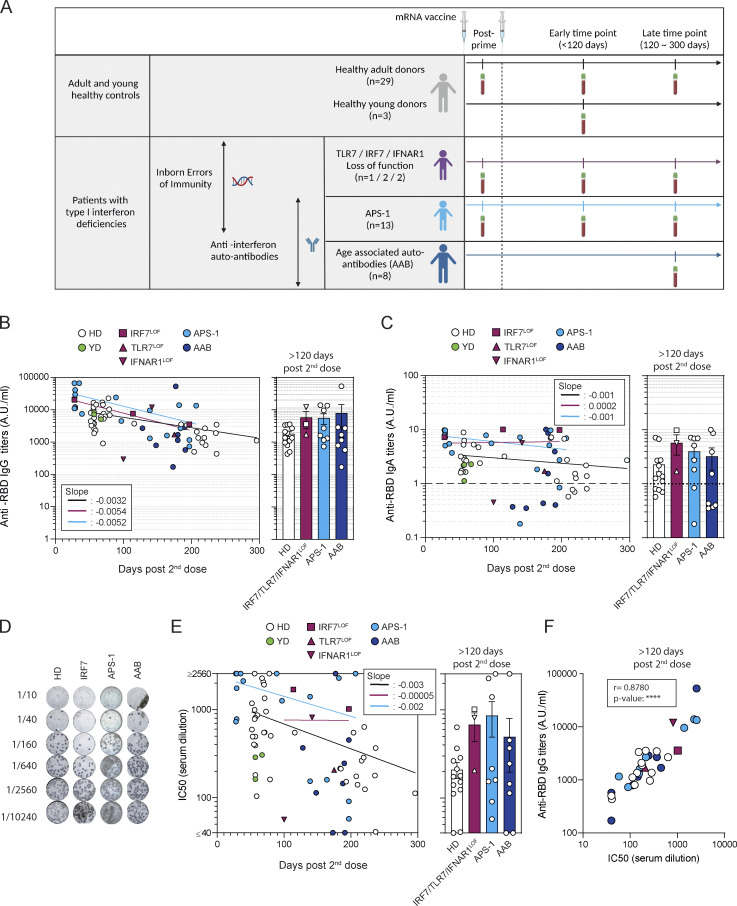
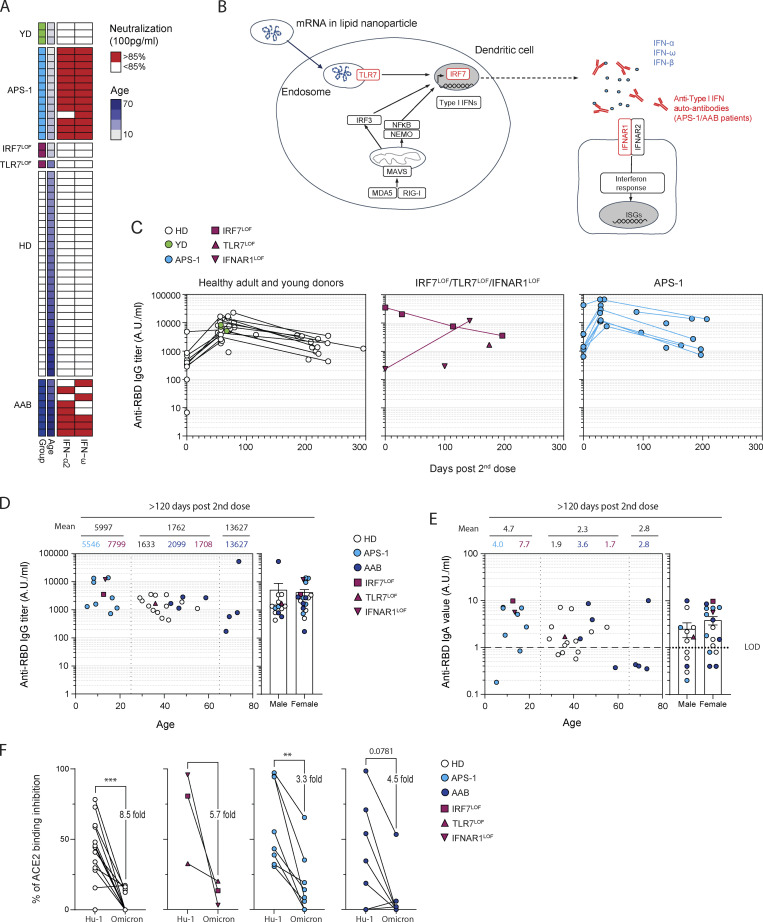
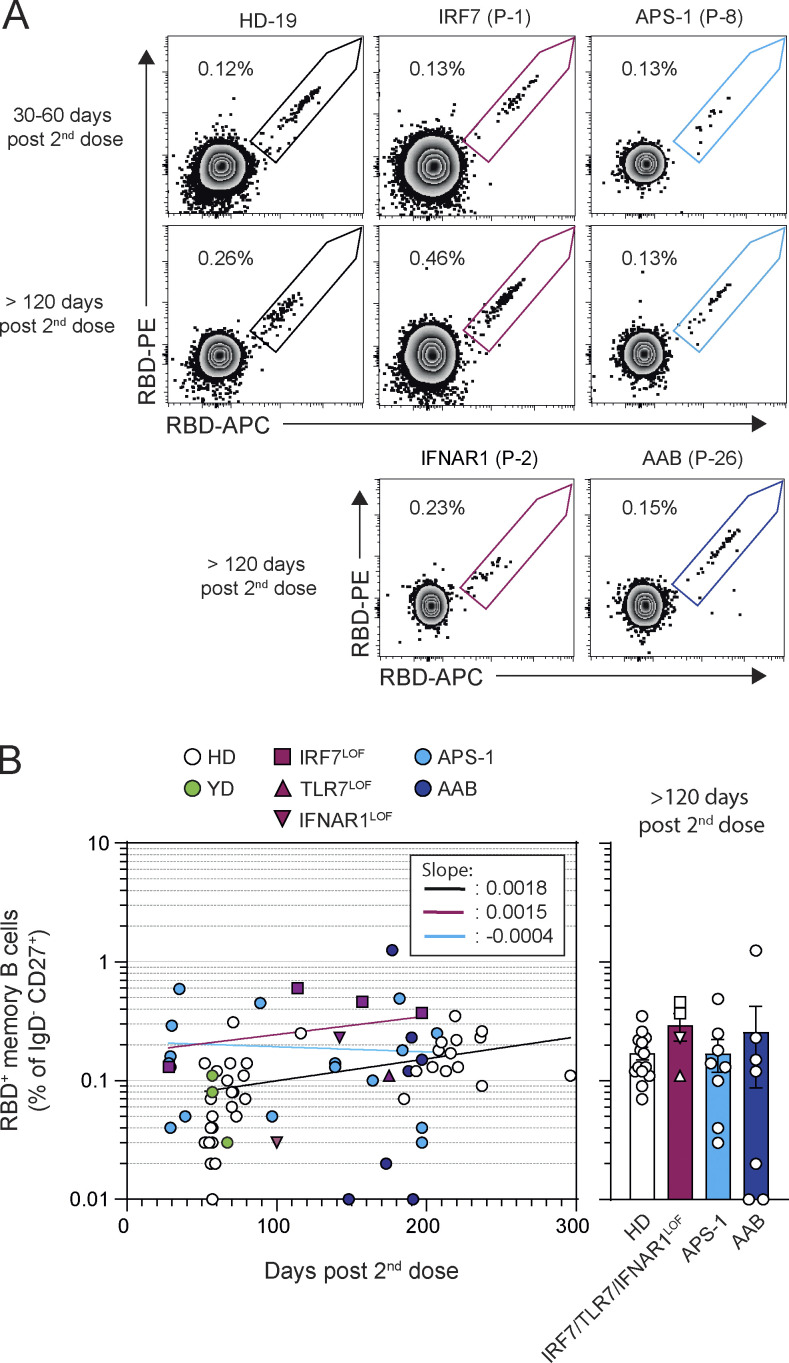
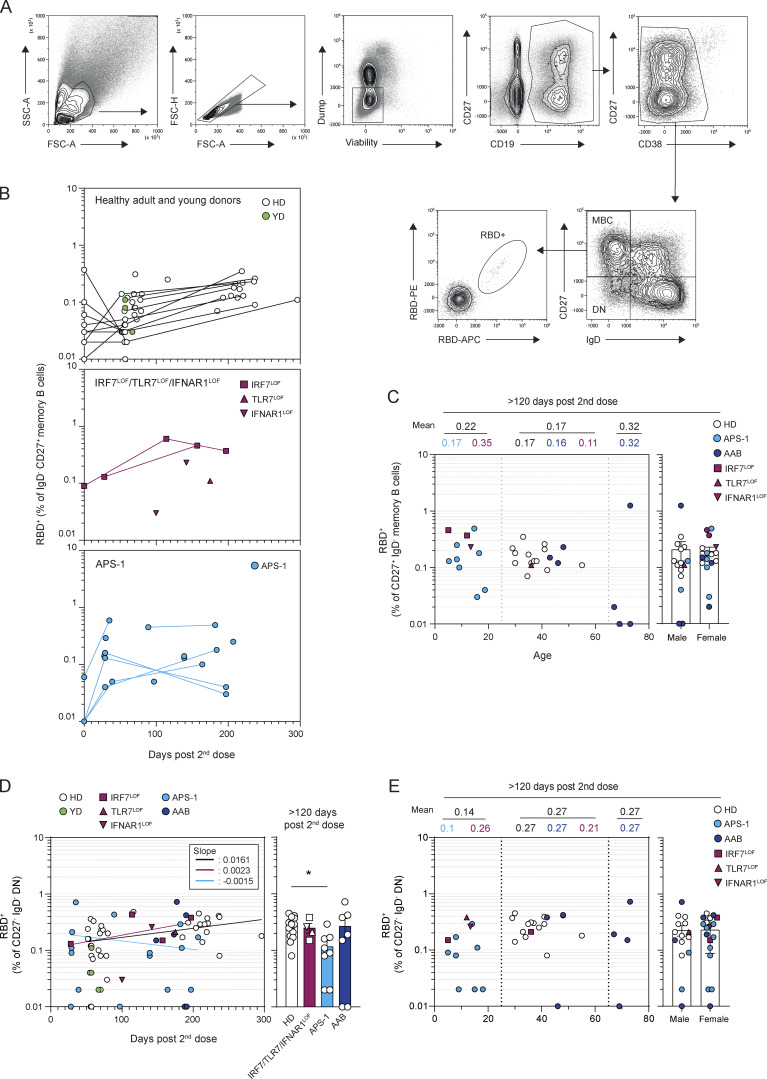
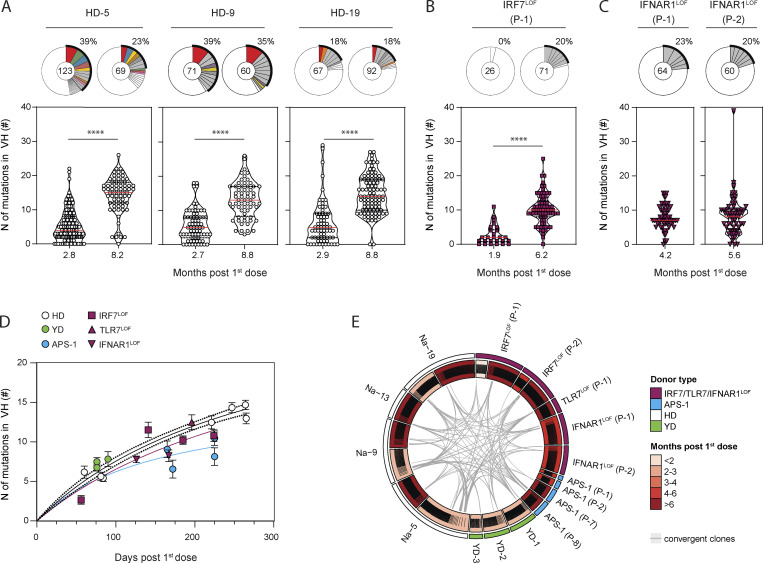
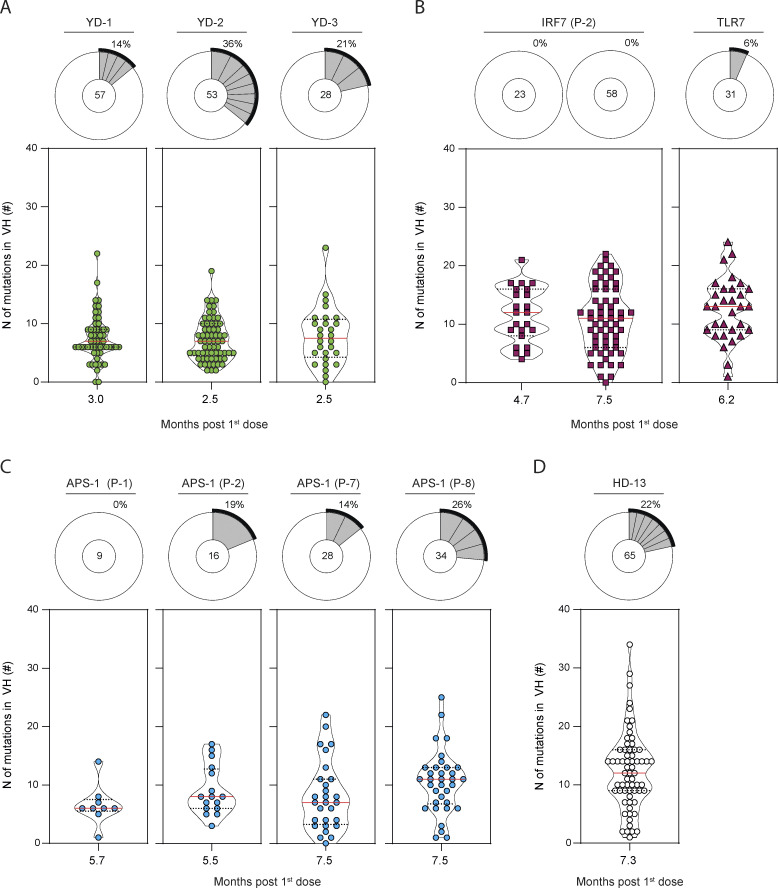
Inborn and acquired deficits of type I interferon (IFN) immunity predispose to life-threatening COVID-19 pneumonia. We longitudinally profiled the B cell response to mRNA vaccination in SARS-CoV-2 naive patients with inherited TLR7, IRF7, or IFNAR1 deficiency, as well as young patients with autoantibodies neutralizing type I IFNs due to autoimmune polyendocrine syndrome type-1 (APS-1) and older individuals with age-associated autoantibodies to type I IFNs. The receptor-binding domain spike protein (RBD)-specific memory B cell response in all patients was quantitatively and qualitatively similar to healthy donors. Sustained germinal center responses led to accumulation of somatic hypermutations in immunoglobulin heavy chain genes. The amplitude and duration of, and viral neutralization by, RBD-specific IgG serological response were also largely unaffected by TLR7, IRF7, or IFNAR1 deficiencies up to 7 mo after vaccination in all patients. These results suggest that induction of type I IFN is not required for efficient generation of a humoral response against SARS-CoV-2 by mRNA vaccines.
Trial registration: ClinicalTrials.gov NCT04402892.
© 2022 Sokal et al.
Conflict of interest statement
Disclosures: S. Fourati reported personal fees from GSK, Cepheid, and Abbott outside the submitted work. I. Meyts reported grants from CSL Behring outside the submitted work. J.-C. Weill received consulting fees from Institut Mérieux. J.-L. Casanova is an inventor on patent application PCT/US2021/042741, filed July 22, 2021, submitted by The Rockefeller University that covers diagnosis of susceptibility to, and treatment of, viral disease and viral vaccines, including COVID-19 and vaccine-associated diseases. M. Mahévas reported grants from GSK and personal fees from Novartis, LFB, and Amgen outside the submitted work. No other disclosures were reported.
Figures
Similar articles
-
Unlocking life-threatening COVID-19 through two types of inborn errors of type I IFNs.J Clin Invest. 2023 Feb 1;133(3):e166283. doi: 10.1172/JCI166283. J Clin Invest. 2023. PMID: 36719370 Free PMC article. Review.
-
High-Resolution Linear Epitope Mapping of the Receptor Binding Domain of SARS-CoV-2 Spike Protein in COVID-19 mRNA Vaccine Recipients.Microbiol Spectr. 2021 Dec 22;9(3):e0096521. doi: 10.1128/Spectrum.00965-21. Epub 2021 Nov 10. Microbiol Spectr. 2021. PMID: 34756082 Free PMC article.
-
Characterization of SARS-CoV-2-Specific Humoral and Cellular Immune Responses Induced by Inactivated COVID-19 Vaccines in a Real-World Setting.Front Immunol. 2021 Dec 22;12:802858. doi: 10.3389/fimmu.2021.802858. eCollection 2021. Front Immunol. 2021. PMID: 35003131 Free PMC article.
-
Cellular and humoral functional responses after BNT162b2 mRNA vaccination differ longitudinally between naive and subjects recovered from COVID-19.Cell Rep. 2022 Jan 11;38(2):110235. doi: 10.1016/j.celrep.2021.110235. Epub 2021 Dec 21. Cell Rep. 2022. PMID: 34986327 Free PMC article.
-
New-onset dermatomyositis following SARS-CoV-2 infection and vaccination: a case-based review.Rheumatol Int. 2022 Dec;42(12):2267-2276. doi: 10.1007/s00296-022-05176-3. Epub 2022 Aug 8. Rheumatol Int. 2022. PMID: 35939078 Free PMC article. Review.
Cited by
-
T-bet+ B cells are activated by and control endogenous retroviruses through TLR-dependent mechanisms.Nat Commun. 2024 Feb 9;15(1):1229. doi: 10.1038/s41467-024-45201-6. Nat Commun. 2024. PMID: 38336876 Free PMC article.
-
Vaccination prevents severe COVID-19 outcome in patients with neutralizing type 1 interferon autoantibodies.iScience. 2023 Jul 21;26(7):107084. doi: 10.1016/j.isci.2023.107084. Epub 2023 Jun 9. iScience. 2023. PMID: 37346050 Free PMC article.
-
No link between type I interferon autoantibody positivity and adverse reactions to COVID-19 vaccines.NPJ Vaccines. 2024 Feb 22;9(1):42. doi: 10.1038/s41541-024-00829-9. NPJ Vaccines. 2024. PMID: 38388530 Free PMC article.
-
Unlocking life-threatening COVID-19 through two types of inborn errors of type I IFNs.J Clin Invest. 2023 Feb 1;133(3):e166283. doi: 10.1172/JCI166283. J Clin Invest. 2023. PMID: 36719370 Free PMC article. Review.
-
Type I interferons induce an epigenetically distinct memory B cell subset in chronic viral infection.Immunity. 2024 May 14;57(5):1037-1055.e6. doi: 10.1016/j.immuni.2024.03.016. Epub 2024 Apr 8. Immunity. 2024. PMID: 38593796
References
-
- Alameh, M.-G., Tombácz I., Bettini E., Lederer K., Sittplangkoon C., Wilmore J.R., Gaudette B.T., Soliman O.Y., Pine M., Hicks P., et al. . 2021. Lipid nanoparticles enhance the efficacy of mRNA and protein subunit vaccines by inducing robust T follicular helper cell and humoral responses. Immunity. 54:2877–2892.e7. 10.1016/j.immuni.2021.11.001 - DOI - PMC - PubMed
-
- Asano, T., Boisson B., Onodi F., Matuozzo D., Moncada-Velez M., Maglorius Renkilaraj M.R.L., Zhang P., Meertens L., Bolze A., Materna M., et al. . 2021. X-linked recessive TLR7 deficiency in ∼1% of men under 60 years old with life-threatening COVID-19. Sci. Immunol. 6:eabl4348. 10.1126/sciimmunol.abl4348 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
