

The Level of Remnant Cholesterol and Implications for Lipid-Lowering Strategy in Hospitalized Patients with Acute Coronary Syndrome in China: Findings from the Improving Care for Cardiovascular Disease in China-Acute Coronary Syndrome Project
- PMID: 36295800
- PMCID: PMC9607962
- DOI: 10.3390/metabo12100898
The Level of Remnant Cholesterol and Implications for Lipid-Lowering Strategy in Hospitalized Patients with Acute Coronary Syndrome in China: Findings from the Improving Care for Cardiovascular Disease in China-Acute Coronary Syndrome Project
Abstract
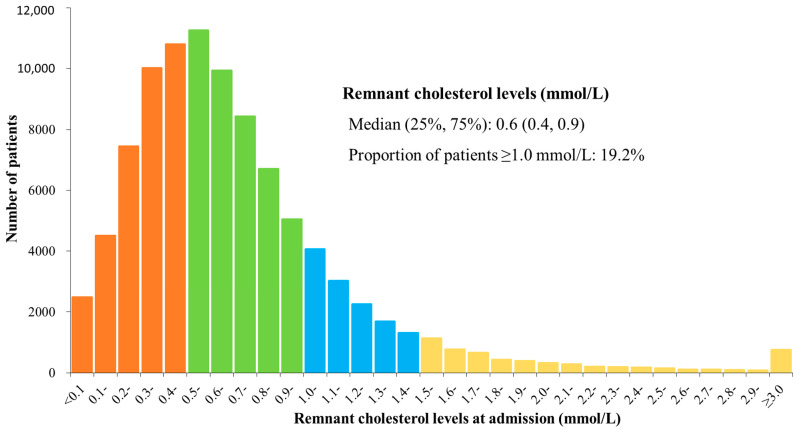
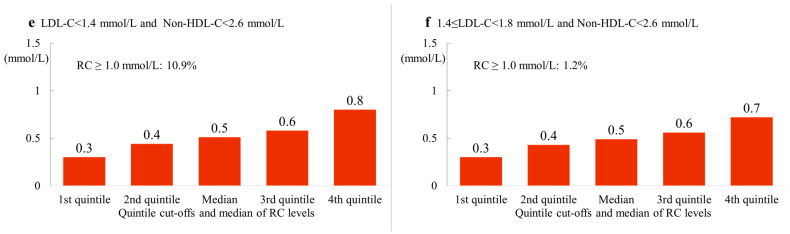
Elevated remnant cholesterol is associated with an increased risk of atherosclerotic cardiovascular disease (ASCVD). We aimed to evaluate the concentrations and general distribution of remnant cholesterol at admission in patients hospitalized for acute coronary syndrome (ACS), and those in patients who reached the low-density lipoprotein cholesterol (LDL-C) target or non-high-density lipoprotein cholesterol (non-HDL-C) target. Patients with ACS who were enrolled in the Improving Care for Cardiovascular Disease in China—ACS project from 2014 to 2019 were included. Elevated remnant cholesterol concentrations were defined as ≥1.0 mmol/L. Among 94,869 patients, the median (interquartile range) remnant cholesterol concentration at admission was 0.6 mmol/L (0.4−0.9 mmol/L) and 19.2% had elevated remnant cholesterol concentrations. Among patients with LDL-C concentrations < 1.4 mmol/L, 24.4% had elevated remnant cholesterol concentrations, while the proportion was 13.3% among patients with LDL-C concentrations between 1.4 and 1.7 mmol/L. Among patients with non-HDL-C concentrations < 2.6 mmol/L, 2.9% had elevated remnant cholesterol concentrations but 79.6% had LDL-C concentrations ≥ 1.4 mmol/L. Even among patients with LDL-C < 1.4 mmol/L and non-HDL-C < 2.6 mmol/L, 10.9% had elevated remnant cholesterol. In conclusion, one fifth of patients with ACS have elevated remnant cholesterol concentrations at admission. Elevated remnant cholesterol concentrations are present in patients with LDL-C or/and non-HDL-C concentrations within the target, which represents an unmet need to add remnant cholesterol as a target for the secondary prevention of ASCVD.
Keywords: acute coronary syndrome; low-density lipoprotein cholesterol; non-high-density lipoprotein cholesterol; remnant cholesterol.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

Similar articles
-
Elevated remnant cholesterol and non-HDL cholesterol concentrations from real-world laboratory results: a cross-sectional study in Southeast Asians.Front Cardiovasc Med. 2024 Feb 7;11:1328618. doi: 10.3389/fcvm.2024.1328618. eCollection 2024. Front Cardiovasc Med. 2024. PMID: 38385128 Free PMC article.
-
[Low-density lipoprotein cholesterol levels and lipid-lowering treatment status among young and middle-aged ultra-high-risk patients with acute coronary syndrome in China].Zhonghua Xin Xue Guan Bing Za Zhi. 2022 Dec 24;50(12):1161-1168. doi: 10.3760/cma.j.cn112148-20220920-00731. Zhonghua Xin Xue Guan Bing Za Zhi. 2022. PMID: 36517436 Chinese.
-
Lowering Targeted Atherogenic Lipoprotein Cholesterol Goals for Patients at "Extreme" ASCVD Risk.Curr Diab Rep. 2019 Nov 21;19(12):146. doi: 10.1007/s11892-019-1246-y. Curr Diab Rep. 2019. PMID: 31754844 Review.
-
[Statin use and low-density lipoprotein cholesterol levels in patients aged 75 years and older with acute coronary syndrome in China].Zhonghua Xin Xue Guan Bing Za Zhi. 2019 May 24;47(5):351-359. doi: 10.3760/cma.j.issn.0253-3758.2019.05.005. Zhonghua Xin Xue Guan Bing Za Zhi. 2019. PMID: 31142078 Chinese.
-
Evolocumab (Repatha): Indication: Repatha is indicated for the reduction of elevated low-density lipoprotein cholesterol in adult patients with primary hyperlipidemia (including heterozygous familial hypercholesterolemia and atherosclerotic cardiovascular disease): as an adjunct to diet and statin therapy, with or without other lipid-lowering therapies, in patients who require additional lowering of low-density lipoprotein cholesterol as an adjunct to diet, alone or in combination with non-statin lipid-lowering therapies, in patients for whom a statin is contraindicated: CADTH Reimbursement Recommendation [Internet].Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2024 Aug. Report No.: SR0821. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2024 Aug. Report No.: SR0821. PMID: 39312596 Free Books & Documents. Review.
Cited by
-
The Role of Triglyceride-rich Lipoproteins and Their Remnants in Atherosclerotic Cardiovascular Disease.Eur Cardiol. 2023 Sep 28;18:e56. doi: 10.15420/ecr.2023.16. eCollection 2023. Eur Cardiol. 2023. PMID: 37860700 Free PMC article. Review.
-
2024 Guidelines of the Polish Society of Laboratory Diagnostics and the Polish Lipid Association on laboratory diagnostics of lipid metabolism disorders.Arch Med Sci. 2024 Mar 18;20(2):357-374. doi: 10.5114/aoms/186191. eCollection 2024. Arch Med Sci. 2024. PMID: 38757022 Free PMC article.
-
Emerging therapies for refractory hypercholesterolemia: a narrative review.Future Cardiol. 2024 Apr 25;20(5-6):317-334. doi: 10.1080/14796678.2024.2367860. Epub 2024 Jul 10. Future Cardiol. 2024. PMID: 38985520 Review.
-
A significant presence in atherosclerotic cardiovascular disease: Remnant cholesterol: A review.Medicine (Baltimore). 2024 Jul 5;103(27):e38754. doi: 10.1097/MD.0000000000038754. Medicine (Baltimore). 2024. PMID: 38968507 Free PMC article. Review.
-
Effects of remnant cholesterol on the efficacy of genotype-guided dual antiplatelet in CYP2C19 loss-of -function carriers with minor stroke or transient ischaemic attack: a post-hoc analysis of the CHANCE-2 trial.EClinicalMedicine. 2023 Dec 2;67:102357. doi: 10.1016/j.eclinm.2023.102357. eCollection 2024 Jan. EClinicalMedicine. 2023. PMID: 38125963 Free PMC article.
References
-
- Roth G.A., Mensah G.A., Johnson C.O., Addolorato G., Ammirati E., Baddour L.M., Barengo N.C., Beaton A.Z., Benjamin E.J., Benziger C.P., et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 Study. J. Am. Coll. Cardiol. 2020;76:2982–3021. doi: 10.1016/j.jacc.2020.11.010. - DOI - PMC - PubMed
-
- Baigent C., Keech A., Kearney P.M., Blackwell L., Buck G., Pollicino C., Kirby A., Sourjina T., Peto R., Collins R., et al. Efficacy and safety of cholesterol-lowering treatment: Prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005;366:1267–1278. - PubMed
-
- Joint Committee on the Revision of Guidelines for prevention and treatment of dyslipidemia in Chinese adults, Guidelines for prevention and treatment of dyslipidemia in Chinese adults (2016 revision) Chin. Circ. J. 2016;31:937–950.
-
- National Clinical Guideline Center . Lipid Modification: Cardiovascular Risk Assessment and the Modification of Blood Lipids for the Primary and Secondary Prevention of Cardiovascular Disease. National Institute for Health and Care Excellence (UK); Copyright © National Clinical Guideline Centre; London, UK: 2014. - PubMed
-
- Handelsman Y., Jellinger P.S., Guerin C.K., Bloomgarden Z.T., Brinton E.A., Budoff M.J., Davidson M.H., Einhorn D., Fazio S., Fonseca V.A., et al. Consensus statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the management of dyslipidemia and prevention of cardiovascular disease algorithm—2020 executive summary. Endocr. Pract. 2020;26:1196–1224. doi: 10.4158/CS-2020-0490. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
