

Diagnostic Accuracy of Ultrasound in Predicting Extrathyroidal Extension and Its Relation to Body Mass Index in a North American Population
- PMID: 36289671
- PMCID: PMC9598864
- DOI: 10.3390/biomedicines10102408
Diagnostic Accuracy of Ultrasound in Predicting Extrathyroidal Extension and Its Relation to Body Mass Index in a North American Population
Abstract
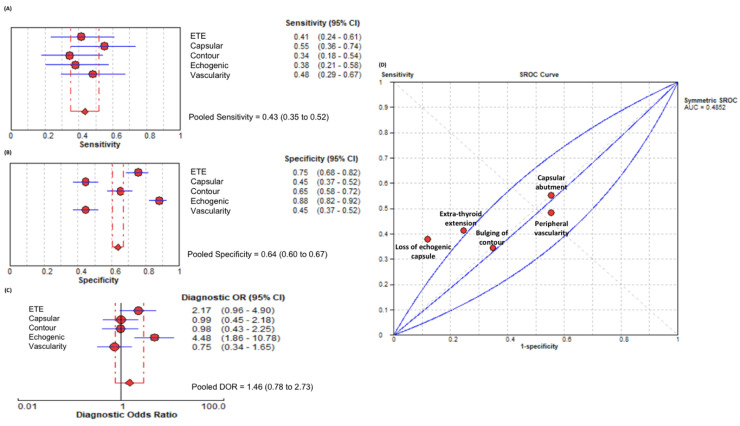
Detection of extrathyroidal extension (ETE) in patients with papillary thyroid carcinoma (PTC) influences treatment plan and surgical aggressiveness. Ultrasound (US) is the long-standing preoperative imaging method of choice. Recent literature from Asia suggests US accuracy to be influenced by patient characteristics, such as body mass index (BMI). Here, we examine the effect of BMI on the accuracy of US at a North American tertiary referral center. A total of 204 PTC-confirmed patients were retrospectively read by a radiologist blinded to surgical pathology findings. The radiologist recorded multiple sonographic features, including ETE, loss of echogenic capsule, nodule vascularity, capsular abutment, and bulging of contour. When considering all patients, the ultrasonographic feature with the best overall performance was loss of echogenic capsule (diagnostic odds ratio (DOR) = 4.48, 95% confidence interval (CI) = 1.86-10.78). Sub-group analysis by patient BMI found that area under the curve (AUC) for sonographic features was greater in non-obese BMI patients (0.71 ± 0.06) when compared with obese patients (0.43 ± 0.05; p = 0.001). Overall, US diagnostic performance was significantly better in non-obese (DOR = 3.70, 95%CI = 1.53-8.94) patients when compared to those who were obese (DOR = 1.12, 95%CI = 0.62-2.03; p = 0.03). Loss of the echogenic capsule did not differ between the two cohorts with respect to DOR (p = 0.51), specificity (p = 0.52), or sensitivity (p = 0.09). Our work suggests that the diagnostic value of ETE detection by US is impaired in obese patients. Considering that loss of the echogenic capsule did not differ with respect to diagnostic performance, specificity, nor sensitivity between non-obese and obese patients, it could be considered the most important predictor of US-determined ETE.
Keywords: ETE; body mass index; extrathyroidal extension; papillary thyroid cancer; ultrasound.
Conflict of interest statement
All authors declare no conflict of interest. The sponsors had no role in the design, execution, interpretation, or writing of the study.
Figures

Similar articles
-
The Diagnostic Performance of Ultrasonography in the Evaluation of Extrathyroidal Extension in Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis.Int J Mol Sci. 2022 Dec 26;24(1):371. doi: 10.3390/ijms24010371. Int J Mol Sci. 2022. PMID: 36613811 Free PMC article. Review.
-
Sonographic Detection of Extracapsular Extension in Papillary Thyroid Cancer.J Ultrasound Med. 2015 Dec;34(12):2225-30. doi: 10.7863/ultra.15.02006. Epub 2015 Oct 30. J Ultrasound Med. 2015. PMID: 26518279
-
[Diagnostic Value of Contrast-enhanced Ultrasound in Extrathyroidal Extension of Papillary Thyroid Carcinoma].Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2020 Oct;42(5):619-625. doi: 10.3881/j.issn.1000-503X.12632. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2020. PMID: 33131516 Chinese.
-
Sonographic assessment of minor extrathyroidal extension of papillary thyroid microcarcinoma involving the posterior thyroid capsule.Eur Radiol. 2022 Sep;32(9):6090-6096. doi: 10.1007/s00330-022-08765-9. Epub 2022 Apr 5. Eur Radiol. 2022. PMID: 35380227
-
Shear wave elastography combined with gray-scale ultrasound for predicting central lymph node metastasis of papillary thyroid carcinoma.Surg Oncol. 2021 Mar;36:1-6. doi: 10.1016/j.suronc.2020.11.004. Epub 2020 Nov 25. Surg Oncol. 2021. PMID: 33271464 Review.
Cited by
-
The Diagnostic Performance of Ultrasonography in the Evaluation of Extrathyroidal Extension in Papillary Thyroid Carcinoma: A Systematic Review and Meta-Analysis.Int J Mol Sci. 2022 Dec 26;24(1):371. doi: 10.3390/ijms24010371. Int J Mol Sci. 2022. PMID: 36613811 Free PMC article. Review.
References
-
- Orlov S., Orlov D., Shaytzag M., Dowar M., Tabatabaie V., Dwek P., Yip J., Hu C., Freeman J.L., Walfish P.G., et al. Influence of Age and Primary Tumor Size on the Risk for Residual/Recurrent Well-differentiated Thyroid Carcinoma. Head Neck J. Sci. Spec. Head Neck. 2009;31:782–788. doi: 10.1002/hed.21020. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
