

Rehabilitation of Airway Protection in Individuals With Movement Disorders: A Telehealth Feasibility Study
- PMID: 36279509
- PMCID: PMC9911128
- DOI: 10.1044/2022_AJSLP-22-00063
Rehabilitation of Airway Protection in Individuals With Movement Disorders: A Telehealth Feasibility Study
Abstract
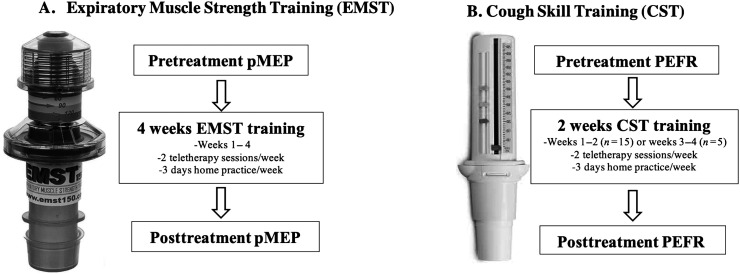
Purpose: Airway protective deficits (swallowing and cough) greatly reduce health and quality of life and are a pervasive consequence of neurodegenerative movement disorders. Expiratory muscle strength training (EMST) and cough skill training (CST) are two treatment approaches to improve airway protection; however, many patients are unable to access these treatments. Telehealth may improve access to care, but it remains unknown whether these treatments are feasible and efficacious via telehealth. This study aimed to determine the practical feasibility and preliminary treatment effect of EMST and CST via telehealth.
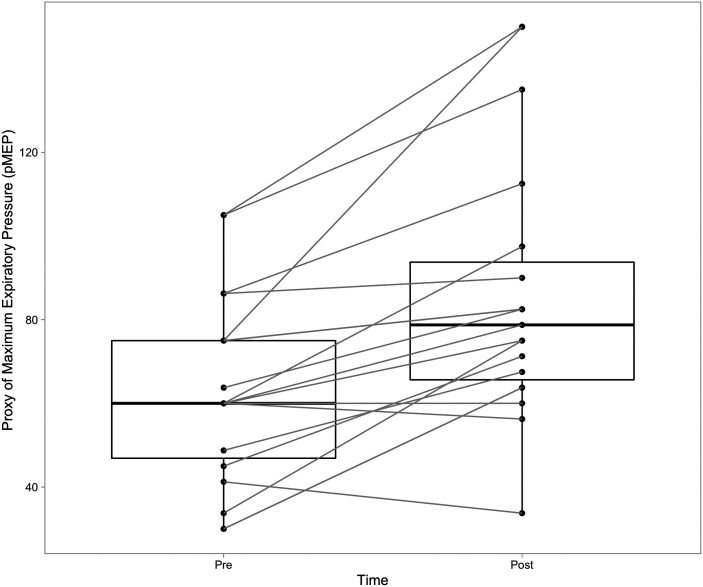
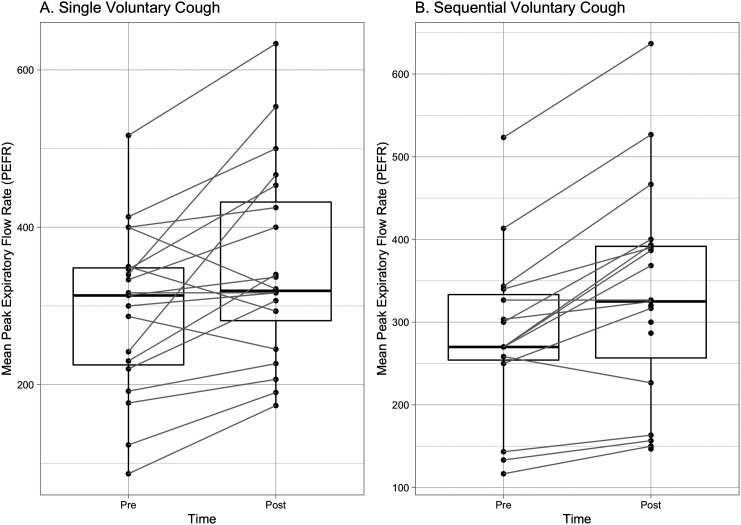
Method: Twenty participants with movement disorders completed 4 weeks of EMST and 2 weeks of CST, including two clinician-directed treatment sessions via telehealth and 3 days of home practice per week. Feasibility was calculated for each treatment. Practical feasibility was defined as completing treatment (EMST or CST) and obtaining the relevant outcome measures-a proxy of maximum expiratory pressure (pMEP) for EMST and peak expiratory flow rate (PEFR) for CST-within a 30-min session/period. Session factors that may have influenced feasibility were examined. Preliminary treatment effect was defined as changes in pMEP and PEFR.
Results: Time taken to obtain pMEP and complete EMST was 17.48 min, and time taken to obtain PEFR and complete CST was 17.69 min. pMEP, single voluntary cough PEFR, and sequential voluntary cough PEFR increased from pre- to posttreatment.
Conclusions: Findings suggest that the delivery of EMST and CST is feasible via telehealth and yield improvements to pMEP and PEFR. This has important implications for expanding service delivery of airway protective interventions and reducing health care disparities in people with neurodegenerative movement disorders.
Supplemental material: https://doi.org/10.23641/asha.21357669.
Figures
Similar articles
-
Rehabilitating Cough Dysfunction in Parkinson's Disease: A Randomized Controlled Trial.Mov Disord. 2023 Feb;38(2):201-211. doi: 10.1002/mds.29268. Epub 2022 Nov 7. Mov Disord. 2023. PMID: 36345090 Clinical Trial.
-
Rehabilitation of Swallowing and Cough Functions Following Stroke: An Expiratory Muscle Strength Training Trial.Arch Phys Med Rehabil. 2016 Aug;97(8):1345-51. doi: 10.1016/j.apmr.2016.03.027. Epub 2016 Apr 26. Arch Phys Med Rehabil. 2016. PMID: 27130637 Clinical Trial.
-
A Preliminary Study of Voluntary Cough Motor Performance and Learning With Skill Training and Biofeedback.J Speech Lang Hear Res. 2024 May 7;67(5):1299-1323. doi: 10.1044/2024_JSLHR-23-00516. Epub 2024 Apr 1. J Speech Lang Hear Res. 2024. PMID: 38557139 Clinical Trial.
-
The use of cough peak flow in the assessment of respiratory function in clinical practice- A narrative literature review.Respir Med. 2022 Mar;193:106740. doi: 10.1016/j.rmed.2022.106740. Epub 2022 Jan 15. Respir Med. 2022. PMID: 35123355 Review.
-
High- and low-intensity expiratory muscle strength training in patients with severe obstructive sleep apnea syndrome using non-invasive mechanical ventilation: A double-blinded, randomized controlled trial.Heart Lung. 2023 Sep-Oct;61:29-36. doi: 10.1016/j.hrtlng.2023.03.009. Epub 2023 Apr 21. Heart Lung. 2023. PMID: 37087896 Review.
Cited by
-
Hypotussic cough in persons with dysphagia: biobehavioral interventions and pathways to clinical implementation.Front Rehabil Sci. 2024 Jun 12;5:1394110. doi: 10.3389/fresc.2024.1394110. eCollection 2024. Front Rehabil Sci. 2024. PMID: 38933659 Free PMC article. Review.
-
Post-Radiotherapy Dysphagia in Head and Neck Cancer: Current Management by Speech-Language Pathologists.Curr Treat Options Oncol. 2024 Jun;25(6):703-718. doi: 10.1007/s11864-024-01198-0. Epub 2024 May 1. Curr Treat Options Oncol. 2024. PMID: 38691257 Free PMC article. Review.
References
-
- Aiello, M. , Rampello, A. , Granella, F. , Maestrelli, M. , Tzani, P. , Immovilli, P. , Franceschini, M. , Olivieri, D. , & Chetta, A. (2008). Cough efficacy is related to the disability status in patients with multiple sclerosis. Respiration, 76(3), 311–316. https://doi.org/10.1159/000119641 - PubMed
-
- Akbar, U. , Dham, B. , He, Y. , Hack, N. , Wu, S. , Troche, M. , Tighe, P. , Nelson, E. , Friedman, J. H. , & Okun, M. S. (2015). Incidence and mortality trends of aspiration pneumonia in Parkinson's disease in the United States, 1979–2010. Parkinsonism & Related Disorders, 21(9), 1082–1086. https://doi.org/10.1016/j.parkreldis.2015.06.020 - PubMed
-
- Anand, S. , El-Bashiti, N. , & Sapienza, C. (2012). Effect of training frequency on maximum expiratory pressure. American Journal of Speech-Language Pathology, 21(4), 380–386. https://doi.org/10.1044/1058-0360(2012/11-0048) - PubMed
-
- Argolo, N. , Sampaio, M. , Pinho, P. , Melo, A. , & Nóbrega, A. C. (2013). Do swallowing exercises improve swallowing dynamic and quality of life in Parkinson's disease? NeuroRehabilitation, 32(4), 949–955. https://doi.org/10.3233/NRE-130918 - PubMed
-
- Athukorala, R. P. , Jones, R. D. , Sella, O. , & Huckabee, M.-L. (2014). Skill training for swallowing rehabilitation in patients with Parkinson's disease. Archives of Physical Medicine and Rehabilitation, 95(7), 1374–1382. https://doi.org/10.1016/j.apmr.2014.03.001 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
