

Relationship Between Preexisting Cardiovascular Disease and Death and Cardiovascular Outcomes in Critically Ill Patients With COVID-19
- PMID: 36193749
- PMCID: PMC9575399
- DOI: 10.1161/CIRCOUTCOMES.122.008942
Relationship Between Preexisting Cardiovascular Disease and Death and Cardiovascular Outcomes in Critically Ill Patients With COVID-19
Abstract
Background: Preexisting cardiovascular disease (CVD) is perceived as a risk factor for poor outcomes in patients with COVID-19. We sought to determine whether CVD is associated with in-hospital death and cardiovascular events in critically ill patients with COVID-19.
Methods: This study used data from a multicenter cohort of adults with laboratory-confirmed COVID-19 admitted to intensive care units at 68 centers across the United States from March 1 to July 1, 2020. The primary exposure was CVD, defined as preexisting coronary artery disease, congestive heart failure, or atrial fibrillation/flutter. Myocardial injury on intensive care unit admission defined as a troponin I or T level above the 99th percentile upper reference limit of normal was a secondary exposure. The primary outcome was 28-day in-hospital mortality. Secondary outcomes included cardiovascular events (cardiac arrest, new-onset arrhythmias, new-onset heart failure, myocarditis, pericarditis, or stroke) within 14 days.
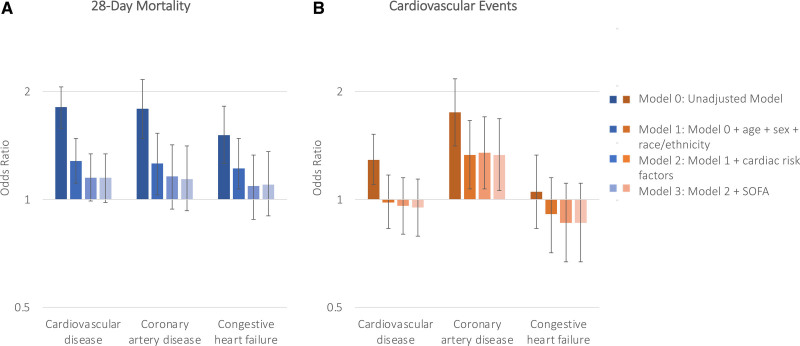
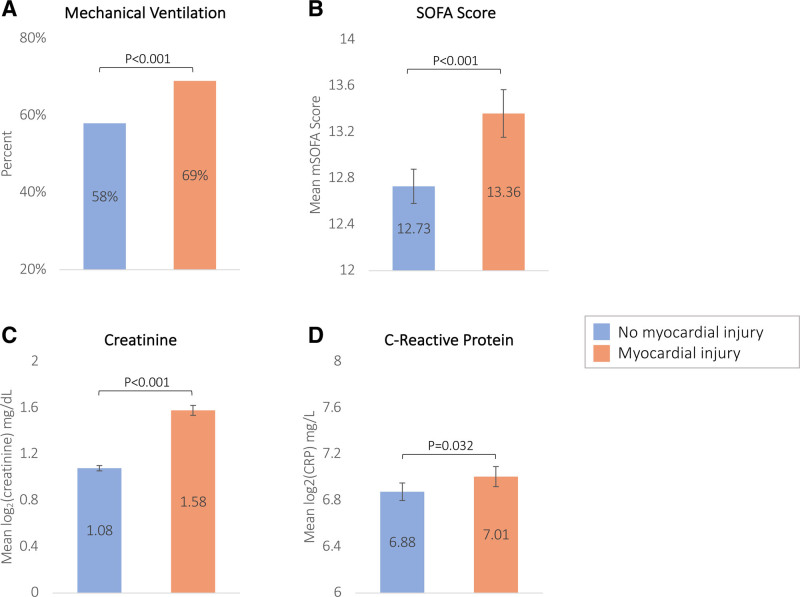
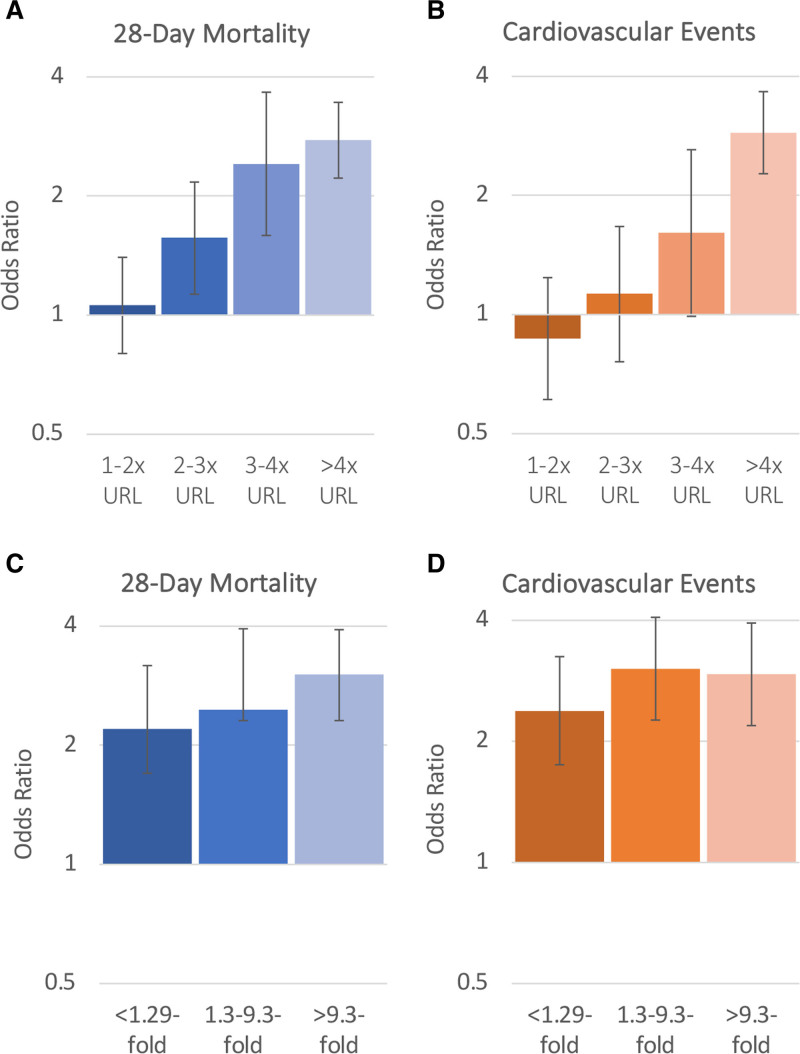
Results: Among 5133 patients (3231 male [62.9%]; mean age 61 years [SD, 15]), 1174 (22.9%) had preexisting CVD. A total of 1178 (34.6%) died, and 920 (17.9%) had a cardiovascular event. After adjusting for age, sex, race, body mass index, history of smoking, and comorbidities, preexisting CVD was associated with a 1.15 (95% CI, 0.98-1.34) higher odds of death. No independent association was observed between preexisting CVD and cardiovascular events. Myocardial injury on intensive care unit admission was associated with higher odds of death (adjusted odds ratio, 1.93 [95% CI, 1.61-2.31]) and cardiovascular events (adjusted odds ratio, 1.82 [95% CI, 1.47-2.24]), regardless of the presence of CVD.
Conclusions: CVD risk factors, rather than CVD itself, were the major contributors to outcomes in critically ill patients with COVID-19. The occurrence of myocardial injury, regardless of CVD, and its association with outcomes suggests it is likely due to multiorgan injury related to acute inflammation rather than exacerbation of preexisting CVD.
Registration: NCT04343898; https://clinicaltrials.gov/ct2/show/NCT04343898.
Keywords: COVID-19; cardiovascular disease; cardiovascular risk factors; inflammation; troponin.
Figures
Similar articles
-
Impact of Cardiovascular Risk Factors and Cardiovascular Diseases on Outcomes in Patients Hospitalized with COVID-19 in Daegu Metropolitan City.J Korean Med Sci. 2021 Jan 11;36(2):e15. doi: 10.3346/jkms.2021.36.e15. J Korean Med Sci. 2021. PMID: 33429474 Free PMC article.
-
Association of Troponin Levels With Mortality in Italian Patients Hospitalized With Coronavirus Disease 2019: Results of a Multicenter Study.JAMA Cardiol. 2020 Nov 1;5(11):1274-1280. doi: 10.1001/jamacardio.2020.3538. JAMA Cardiol. 2020. PMID: 32845276 Free PMC article.
-
Relationship Between Azithromycin and Cardiovascular Outcomes in Unvaccinated Patients With COVID-19 and Preexisting Cardiovascular Disease.J Am Heart Assoc. 2023 Jul 18;12(14):e028939. doi: 10.1161/JAHA.122.028939. Epub 2023 Jul 14. J Am Heart Assoc. 2023. PMID: 37449568 Free PMC article. Clinical Trial.
-
Smoking cessation for secondary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2022 Aug 8;8(8):CD014936. doi: 10.1002/14651858.CD014936.pub2. Cochrane Database Syst Rev. 2022. PMID: 35938889 Free PMC article. Review.
-
Effects of a gluten-reduced or gluten-free diet for the primary prevention of cardiovascular disease.Cochrane Database Syst Rev. 2022 Feb 24;2(2):CD013556. doi: 10.1002/14651858.CD013556.pub2. Cochrane Database Syst Rev. 2022. PMID: 35199850 Free PMC article. Review.
Cited by
-
Thirty-Day Cardiovascular Readmissions Following Discharge with COVID-19: A US Nationwide Readmission Database Analysis from the Pandemic Year 2020.CJC Open. 2023 May 4;5(7):554-66. doi: 10.1016/j.cjco.2023.04.007. Online ahead of print. CJC Open. 2023. PMID: 37362314 Free PMC article.
-
Myocarditis related SARS-CoV-2 infection or vaccination: an expert consensus statement on its diagnosis and management.Rev Esp Cardiol (Engl Ed). 2023 Jul;76(7):555-563. doi: 10.1016/j.rec.2023.01.011. Epub 2023 Mar 11. Rev Esp Cardiol (Engl Ed). 2023. PMID: 36914023 Free PMC article.
-
Association between pre-existing cardiovascular disease, mortality and cardiovascular outcomes in hospitalised patients with COVID-19.Front Cardiovasc Med. 2023 Jul 5;10:1224886. doi: 10.3389/fcvm.2023.1224886. eCollection 2023. Front Cardiovasc Med. 2023. PMID: 37476577 Free PMC article.
-
Factors associated with the outcome of patients with COVID-19 requiring mechanical ventilation: A single-center observational study in Japan.Acute Med Surg. 2023 Jul 8;10(1):e868. doi: 10.1002/ams2.868. eCollection 2023 Jan-Dec. Acute Med Surg. 2023. PMID: 37424772 Free PMC article.
-
Bioinformatics and systems biology approaches to identify molecular targeting mechanism influenced by COVID-19 on heart failure.Front Immunol. 2022 Nov 7;13:1052850. doi: 10.3389/fimmu.2022.1052850. eCollection 2022. Front Immunol. 2022. PMID: 36420258 Free PMC article.
References
-
- John Hopkins University Coronavirus Resource Center. COVID-19 United states cases by county by the Center for Systems Science and Engineering (CSSE) at Johns Hopskins Univeristy. Available at https://coronavirus.jhu.edu/us-map. Accessed July 14, 2022.
-
- Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the chinese center for disease control and prevention. JAMA. 2020;323:1239–1242. doi: 10.1001/jama.2020.2648 - PubMed
-
- Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of coronavirus disease 2019 (COVID-19): a review. JAMA. 2020;324:782–793. doi: 10.1001/jama.2020.12839 - PubMed
-
- Richardson S, Hirsch JS, Narasimhan M, Crawford JM, McGinn T, Davidson KW, Barnaby DP, Becker LB, Chelico JD, Cohen SL, et al. ; the Northwell COVID-19 Research Consortium. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York city area. JAMA. 2020;323:2052–2059. doi: 10.1001/jama.2020.6775 - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
