

Surgical approaches to intramedullary spinal cord astrocytomas in the age of genomics
- PMID: 36147920
- PMCID: PMC9485889
- DOI: 10.3389/fonc.2022.982089
Surgical approaches to intramedullary spinal cord astrocytomas in the age of genomics
Abstract
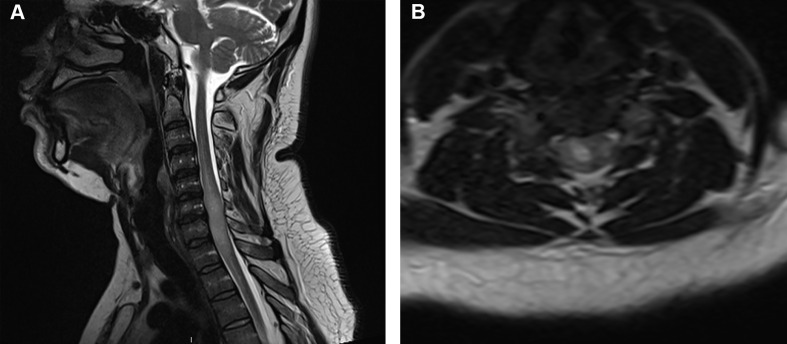
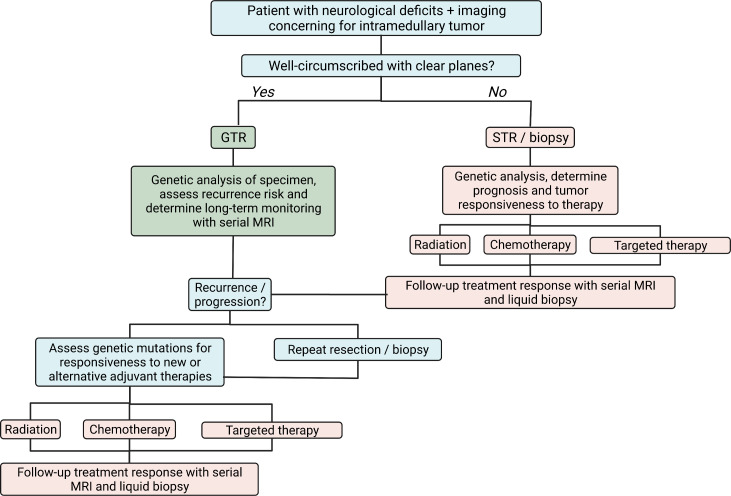
Intramedullary astrocytomas represent approximately 30%-40% of all intramedullary tumors and are the most common intramedullary tumor in children. Surgical resection is considered the mainstay of treatment in symptomatic patients with neurological deficits. Gross total resection (GTR) can be difficult to achieve as astrocytomas frequently present as diffuse lesions that infiltrate the cord. Therefore, GTR carries a substantial risk of new post-operative deficits. Consequently, subtotal resection and biopsy are often the only surgical options attempted. A midline or paramedian sulcal myelotomy is frequently used for surgical resection, although a dorsal root entry zone myelotomy can be used for lateral tumors. Intra-operative neuromonitoring using D-wave integrity, somatosensory, and motor evoked potentials is critical to facilitating a safe resection. Adjuvant radiation and chemotherapy, such as temozolomide, are often administered for high-grade recurrent or progressive lesions; however, consensus is lacking on their efficacy. Biopsied tumors can be analyzed for molecular markers that inform clinicians about the tumor's prognosis and response to conventional as well as targeted therapeutic treatments. Stratification of intramedullary tumors is increasingly based on molecular features and mutational status. The landscape of genetic and epigenetic mutations in intramedullary astrocytomas is not equivalent to their intracranial counterparts, with important difference in frequency and type of mutations. Therefore, dedicated attention is needed to cohorts of patients with intramedullary tumors. Targeted therapeutic agents can be designed and administered to patients based on their mutational status, which may be used in coordination with traditional surgical resection to improve overall survival and functional status.
Keywords: astrocytoma; biomarkers; genetic; intramedullary; resection; spinal cord; targeted therapy; tumor.
Copyright © 2022 Hersh, Jallo and Shimony.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Surgical outcomes of pediatric spinal cord astrocytomas: systematic review and meta-analysis.J Neurosurg Pediatr. 2018 Oct;22(4):404-410. doi: 10.3171/2018.4.PEDS17587. Epub 2018 Jul 20. J Neurosurg Pediatr. 2018. PMID: 30028275
-
Utility of neurophysiological monitoring using dorsal column mapping in intramedullary spinal cord surgery.J Neurosurg Spine. 2010 Jun;12(6):623-8. doi: 10.3171/2010.1.SPINE09112. J Neurosurg Spine. 2010. PMID: 20515347
-
The Role of Radiotherapy, Chemotherapy, and Targeted Therapies in Adult Intramedullary Spinal Cord Tumors.Cancers (Basel). 2024 Aug 6;16(16):2781. doi: 10.3390/cancers16162781. Cancers (Basel). 2024. PMID: 39199553 Free PMC article. Review.
-
Intraoperative changes in transcranial motor evoked potentials and somatosensory evoked potentials predicting outcome in children with intramedullary spinal cord tumors.J Neurosurg Pediatr. 2014 Jun;13(6):591-9. doi: 10.3171/2014.2.PEDS1392. Epub 2014 Apr 4. J Neurosurg Pediatr. 2014. PMID: 24702615 Free PMC article.
-
Neuromonitoring for Intramedullary Spinal Cord Tumor Surgery.World Neurosurg. 2016 Nov;95:108-116. doi: 10.1016/j.wneu.2016.07.066. Epub 2016 Jul 26. World Neurosurg. 2016. PMID: 27474459 Review.
Cited by
-
Case report: Surgical treatment of an astrocytoma in the thoracic spinal cord of a cat.Front Vet Sci. 2023 Oct 24;10:1264916. doi: 10.3389/fvets.2023.1264916. eCollection 2023. Front Vet Sci. 2023. PMID: 37941813 Free PMC article.
-
The disparity in pediatric spinal cord tumor clinical trials: A scoping review of registered clinical trials from 1989 to 2023.Neurooncol Pract. 2024 May 17;11(5):532-545. doi: 10.1093/nop/npae041. eCollection 2024 Oct. Neurooncol Pract. 2024. PMID: 39279782 Review.
-
Astrocytomas of the spinal cord.Neurooncol Adv. 2024 Feb 13;6(Suppl 3):iii48-iii56. doi: 10.1093/noajnl/vdad166. eCollection 2024 Oct. Neurooncol Adv. 2024. PMID: 39430394 Free PMC article. Review.
-
Management and Outcome of Recurring Low-Grade Intramedullary Astrocytomas.Cancers (Basel). 2024 Jun 30;16(13):2417. doi: 10.3390/cancers16132417. Cancers (Basel). 2024. PMID: 39001480 Free PMC article.
-
Intramedullary pediatric low-grade glioma of the spine.Childs Nerv Syst. 2024 Oct;40(10):3107-3117. doi: 10.1007/s00381-024-06499-1. Epub 2024 Jun 21. Childs Nerv Syst. 2024. PMID: 38904769 Review.
References
Publication types
LinkOut - more resources
Full Text Sources