

Enriching the American Heart Association COVID-19 Cardiovascular Disease Registry Through Linkage With External Data Sources: Rationale and Design
- PMID: 36102226
- PMCID: PMC9683646
- DOI: 10.1161/JAHA.122.027094
Enriching the American Heart Association COVID-19 Cardiovascular Disease Registry Through Linkage With External Data Sources: Rationale and Design
Abstract
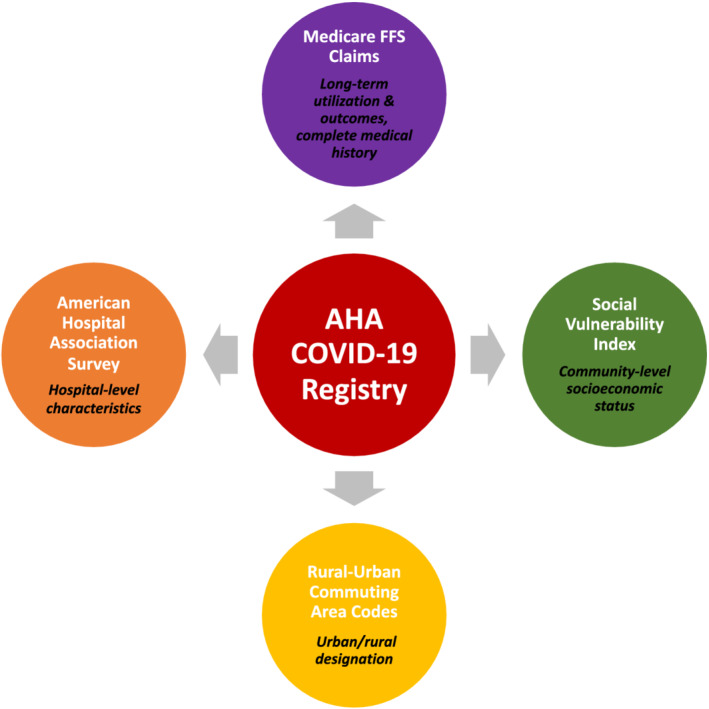
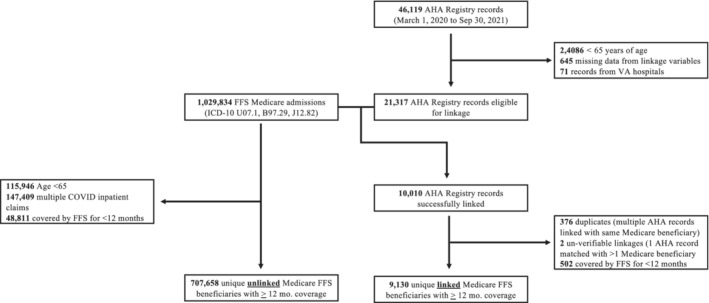
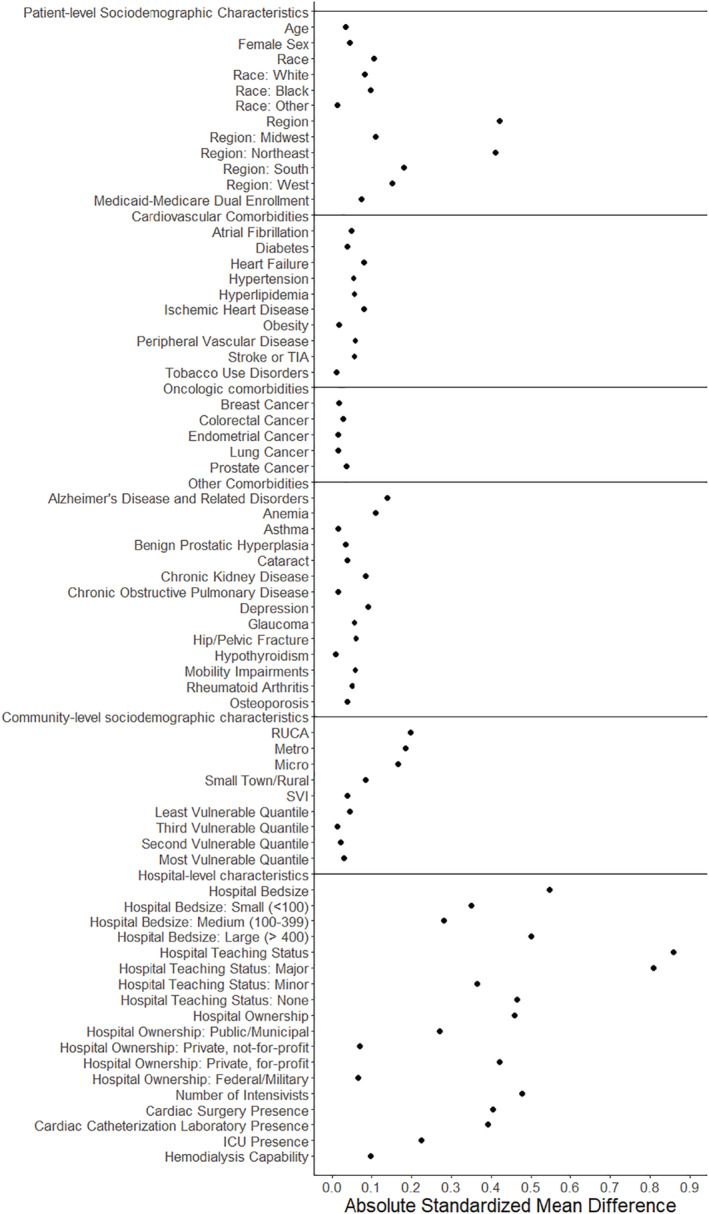
Background The AHA Registry (American Heart Association COVID-19 Cardiovascular Disease Registry) captures detailed information on hospitalized patients with COVID-19. The registry, however, does not capture information on social determinants of health or long-term outcomes. Here we describe the linkage of the AHA Registry with external data sources, including fee-for-service (FFS) Medicare claims, to fill these gaps and assess the representativeness of linked registry patients to the broader Medicare FFS population hospitalized with COVID-19. Methods and Results We linked AHA Registry records of adults ≥65 years from March 2020 to September 2021 with Medicare FFS claims using a deterministic linkage algorithm and with the American Hospital Association Annual Survey, Rural Urban Commuting Area codes, and the Social Vulnerability Index using hospital and geographic identifiers. We compared linked individuals with unlinked FFS beneficiaries hospitalized with COVID-19 to assess the representativeness of the AHA Registry. A total of 10 010 (47.0%) records in the AHA Registry were successfully linked to FFS Medicare claims. Linked and unlinked FFS beneficiaries were similar with respect to mean age (78.1 versus 77.9, absolute standardized difference [ASD] 0.03); female sex (48.3% versus 50.2%, ASD 0.04); Black race (15.1% versus 12.0%, ASD 0.09); dual-eligibility status (26.1% versus 23.2%, ASD 0.07); and comorbidity burden. Linked patients were more likely to live in the northeastern United States (35.7% versus 18.2%, ASD 0.40) and urban/metropolitan areas (83.9% versus 76.8%, ASD 0.18). There were also differences in hospital-level characteristics between cohorts. However, in-hospital outcomes were similar (mortality, 23.3% versus 20.1%, ASD 0.08; home discharge, 45.5% versus 50.7%, ASD 0.10; skilled nursing facility discharge, 24.4% versus 22.2%, ASD 0.05). Conclusions Linkage of the AHA Registry with external data sources such as Medicare FFS claims creates a unique and generalizable resource to evaluate long-term health outcomes after COVID-19 hospitalization.
Keywords: COVID‐19; cardiovascular diseases; fee‐for‐service; medicare; mortality; postdischarge outcomes; readmissions.
Figures
Similar articles
-
Linking a Total Ankle Arthroplasty Registry to Medicare Inpatient Claims without Unique Identifiers.J Bone Joint Surg Am. 2018 Jun 20;100(12):1016-1022. doi: 10.2106/JBJS.17.00460. J Bone Joint Surg Am. 2018. PMID: 29916928
-
Inpatient Utilization and Costs for Medicare Fee-for-Service Beneficiaries with Heart Failure.Am Health Drug Benefits. 2016 Apr;9(2):96-104. Am Health Drug Benefits. 2016. PMID: 27182428 Free PMC article.
-
Comparing post-acute rehabilitation use, length of stay, and outcomes experienced by Medicare fee-for-service and Medicare Advantage beneficiaries with hip fracture in the United States: A secondary analysis of administrative data.PLoS Med. 2018 Jun 26;15(6):e1002592. doi: 10.1371/journal.pmed.1002592. eCollection 2018 Jun. PLoS Med. 2018. PMID: 29944655 Free PMC article.
-
Representativeness of the Get With The Guidelines-Stroke Registry: comparison of patient and hospital characteristics among Medicare beneficiaries hospitalized with ischemic stroke.Stroke. 2012 Jan;43(1):44-9. doi: 10.1161/STROKEAHA.111.626978. Epub 2011 Oct 6. Stroke. 2012. PMID: 21980197
-
American Heart Association COVID-19 CVD Registry Powered by Get With The Guidelines.Circ Cardiovasc Qual Outcomes. 2020 Aug;13(8):e006967. doi: 10.1161/CIRCOUTCOMES.120.006967. Epub 2020 Jun 17. Circ Cardiovasc Qual Outcomes. 2020. PMID: 32546000 Free PMC article. Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
