

Serum level of total histone 3, H3K4me3, and H3K27ac after non-emergent cardiac surgery suggests the persistence of smoldering inflammation at 3 months in an adult population
- PMID: 36068552
- PMCID: PMC9446722
- DOI: 10.1186/s13148-022-01331-6
Serum level of total histone 3, H3K4me3, and H3K27ac after non-emergent cardiac surgery suggests the persistence of smoldering inflammation at 3 months in an adult population
Abstract
Background: Despite clinical relevance of immunological activation due to histone leakage into the serum following cardiac surgery, long-term data describing their longitudinal dynamic are lacking. Therefore, this study examines the serum levels of histone 3 (tH3) and its modifications (H3K4me3 and H3K27ac) alongside immune system activation during the acute and convalescence phases of cardiac surgery.
Methods: Blood samples from fifty-nine individuals were collected before non-emergent cardiac surgery (tpre-op) and 24 h (t24hr), seven days (t7d), and three months (t3m) post-procedure to examine serum levels of tH3, H3K4me3, and H3K27ac. Serum heat shock protein-60 (HSP-60) was a surrogate of the cellular damage marker. Serum C-reactive protein (CRP) and interleukin 6 (IL-6) assessed smoldering inflammation. TNFα and IL-6 production by whole blood in response to lipopolysaccharide (LPS) evaluated immunological activation. Electronic medical records provided demographic, peri-operative, and clinical information. Paired longitudinal analyses were employed with data expressed as mean and standard deviation (X ± SD) or median and interquartile range (Me[IQ25; 75%].
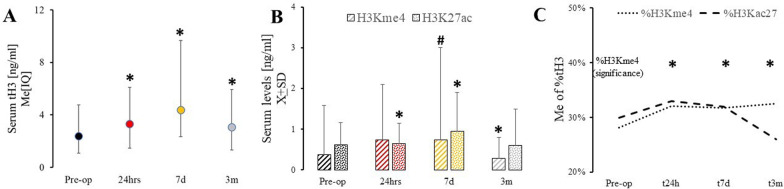
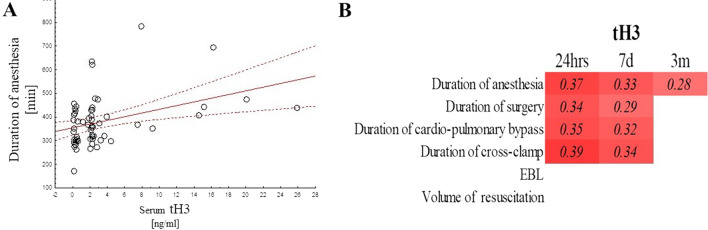
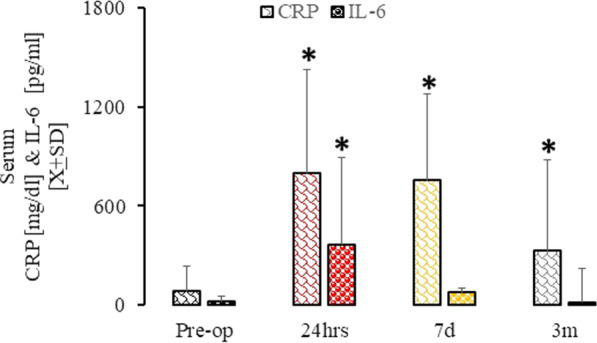
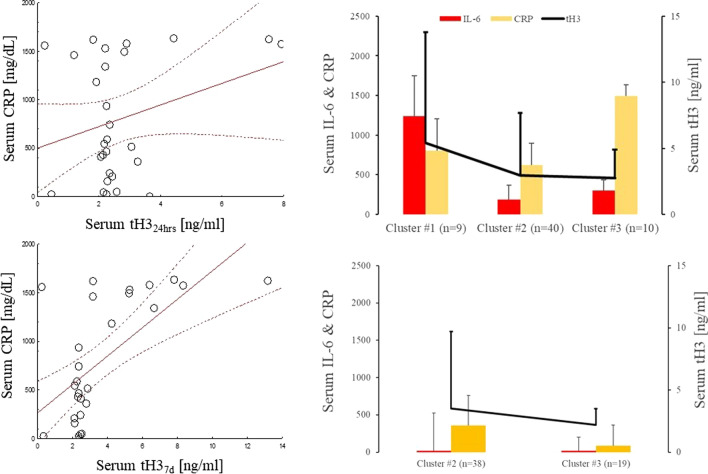
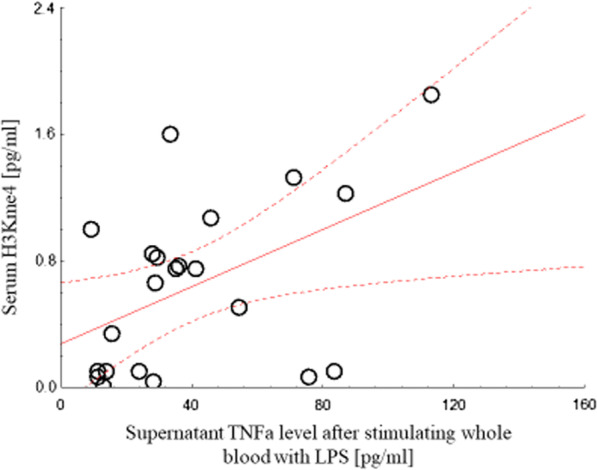
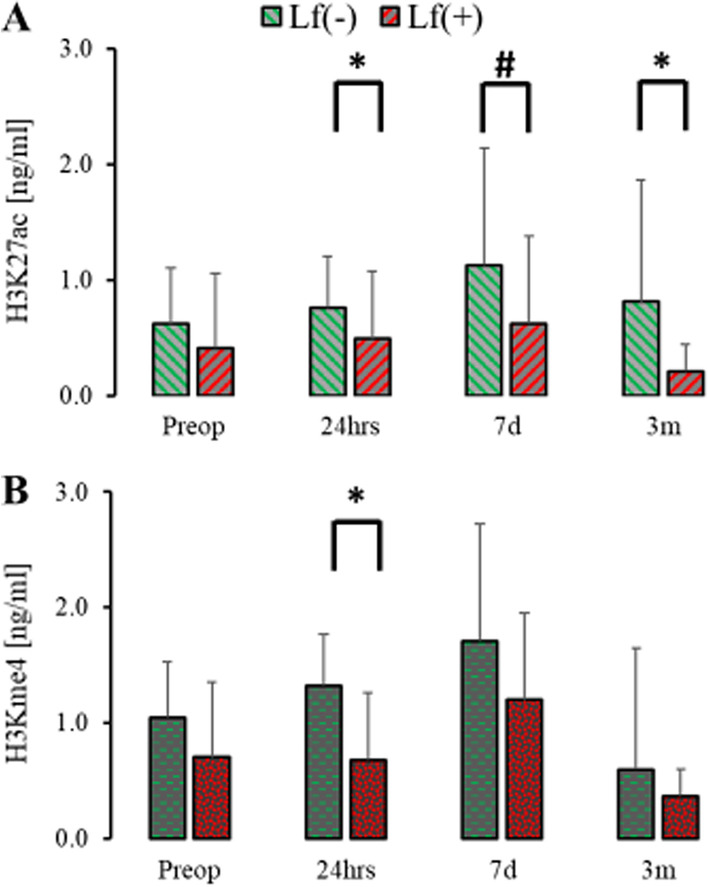
Results: Compared to pre-operative levels (tH3Pre-op = 1.6[0.33;2.4]), post-operative serum tH3 significantly (p > 0.0001) increased after heart surgery (tH324hr = 2.2[0.3;28]), remained elevated at 7 days (tH37d = 2.4[0.37;5.3]), and at 3 months (tH33m = 2.0[0.31;2.9]). Serum H3K27ac was elevated at 24 h (H3K27ac24hr = 0.66 ± 0.51; p = 0.025) and seven days (H3K27ac7d = 0.94 ± 0.95; p = 0.032) as compared to baseline hours (H3K27acPre-op = 0.55 ± 0.54). Serum H3K4me3 was significantly diminished at three months (H3K4me3Pre-op = 0.94 ± 0.54 vs. H3K27ac3m = 0.59 ± 0.89; p = 0.008). tH3 correlated significantly with the duration of anesthesia (r2 = 0.38). In contrast, HSP-60 normalized seven days after surgery. Peri-operative intake of acetaminophen, but no acetylsalicylic acid (ASA), acid, ketorolac or steroids, resulted in the significant depression of serum H3K4me3 at 24 h (H3K4me3acetom- = 1.26[0.71; 3.21] vs H3K4me3acetom+ = 0.54[0.07;1.01]; W[50] = 2.26; p = 0.021). CRP, but not IL-6, remained elevated at 3 months compared to pre-surgical levels and correlated with tH324hrs (r2 = 0.43), tH37d (r2 = 0.71; p < 0.05), H3K4me37d (r2 = 0.53), and H3K27ac7d (r2 = 0.49). Production of TNFα by whole blood in response to LPS was associated with serum tH324hrs (r2 = 0.67). Diminished H3K4me324hrs, H3K27ac24hrs, and H3K27ac3m, accompanied the emergence of liver failure.
Conclusions: We demonstrated a prolonged elevation in serum histone 3 three months after cardiac surgery. Furthermore, histone 3 modifications had a discrete time evolution indicating differential immune activation.
Keywords: Acetaminophen; Cardiac surgery; H3K427ac; H3K4me3; Histone 3; Long-term outcome; Smoldering inflammation.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Concomitant elevated serum levels of tenascin, MMP-9 and YKL-40, suggest ongoing remodeling of the heart up to 3 months after cardiac surgery after normalization of the revascularization markers.Eur J Med Res. 2022 Oct 21;27(1):208. doi: 10.1186/s40001-022-00831-8. Eur J Med Res. 2022. PMID: 36271425 Free PMC article.
-
A decline of protective apolipoprotein J and complement factor H concomitant with increase in C5a 3 months after cardiac surgery-Evidence of long-term complement perturbations.Front Cardiovasc Med. 2022 Dec 20;9:983617. doi: 10.3389/fcvm.2022.983617. eCollection 2022. Front Cardiovasc Med. 2022. PMID: 36606279 Free PMC article.
-
Observational study of long-term persistent elevation of neurodegeneration markers after cardiac surgery.Sci Rep. 2019 May 9;9(1):7177. doi: 10.1038/s41598-019-42351-2. Sci Rep. 2019. PMID: 31073130 Free PMC article.
-
Postoperative Dynamic of Leptin and Fibroblast Growth Factor 21 in 123 Patients Recovering from Cardiac Surgery.Med Sci Monit. 2022 Sep 29;28:e937652. doi: 10.12659/MSM.937652. Med Sci Monit. 2022. PMID: 36171690 Free PMC article.
-
Whole Blood Reactivity to Viral and Bacterial Pathogens after Non-Emergent Cardiac Surgery during the Acute and Convalescence Periods Demonstrates a Distinctive Profile of Cytokines Production Compared to the Preoperative Baseline in Cohort of 108 Patients, Suggesting Immunological Reprogramming during the 28 Days Traditionally Recognized as the Post-Surgical Recovery Period.Biomedicines. 2023 Dec 21;12(1):28. doi: 10.3390/biomedicines12010028. Biomedicines. 2023. PMID: 38275389 Free PMC article.
References
-
- Day JR, Taylor KM. The systemic inflammatory response syndrome and cardiopulmonary bypass. Int J Surg. 2005;3:129–140. - PubMed
-
- Giacinto O, Satriano U, Nenna A, Spadaccio C, Lusini M, Mastroianni C, Nappi F, Chello M. Inflammatory response and endothelial dysfunction following cardiopulmonary bypass: pathophysiology and pharmacological targets. Recent Pat Inflamm Allergy Drug Discov. 2019;13:158–173. - PubMed
-
- Ruifrok WT, Westenbrink BD, de Boer RA, den Hamer IJ, Erasmus ME, Mungroop HE, Epema AH, Voors AA, van Veldhuisen DJ, van Gilst WH. Apoptosis during CABG surgery with the use of cardiopulmonary bypass is prominent in ventricular but not in atrial myocardium. Neth Heart J. 2010;18:236–242. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
