

Brain tumor related epilepsy: pathophysiological approaches and rational management of antiseizure medication
- PMID: 36059029
- PMCID: PMC9442934
- DOI: 10.1186/s42466-022-00205-9
Brain tumor related epilepsy: pathophysiological approaches and rational management of antiseizure medication
Abstract
Background: Brain tumor related epilepsy (BTRE) is a common complication of cerebral tumors and its incidence is highly dependent on the type of tumor, ranging from 10-15% in brain metastases to > 80% in low grade gliomas. Clinical management is challenging and has to take into account aspects beyond the treatment of non-tumoral epilepsy.
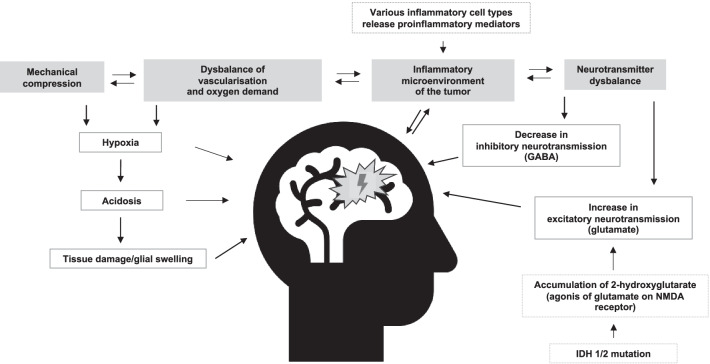
Main body: Increasing knowledge about the pathophysiology of BTRE, particularly on glutamatergic mechanisms of oncogenesis and epileptogenesis, might influence management of anti-tumor and BTRE treatment in the future. The first seizure implies the diagnosis of epilepsy in patients with brain tumors. Due to the lack of prospective randomized trials in BTRE, general recommendations for focal epilepsies currently apply concerning the initiation of antiseizure medication (ASM). Non-enzyme inducing ASM is preferable. Prospective trials are needed to evaluate, if AMPA inhibitors like perampanel possess anti-tumor effects. ASM withdrawal has to be weighed very carefully against the risk of seizure recurrence, but can be achievable in selected patients. Permission to drive is possible for some patients with BTRE under well-defined conditions, but requires thorough neurological, radiological, ophthalmological and neuropsychological examination.
Conclusion: An evolving knowledge on pathophysiology of BTRE might influence future therapy. Randomized trials on ASM in BTRE with reliable endpoints are needed. Management of withdrawal of ASMs and permission to drive demands thorough diagnostic as well as neurooncological and epileptological expertise.
Keywords: Antiseizure medication; Brain metastasis; Brain tumor related epilepsy; Glioma.
© 2022. The Author(s).
Conflict of interest statement
T.W. has received of honoraria or consultation fees Eisai, UCB, GW, Angelini, Precisis and is a stock shareholder of Amgen. J.W. has received speaker fees from UCB, Eisai, Bial, GW pharmaceuticals, and Desitin. U.S. received speaker’s honoraria from Medac, GSK and Novartis. W.G. has received speaker´s honoraria, travel or accommodation payment fees from UCB, Eisei, Bial and Desitin. The other authors declare no competing interests.
Figures
Similar articles
-
Management of brain tumour related epilepsy (BTRE): a narrative review and therapy recommendations.Br J Neurosurg. 2023 Jan 24:1-8. doi: 10.1080/02688697.2023.2170326. Online ahead of print. Br J Neurosurg. 2023. PMID: 36694327 Review.
-
Perampanel in Brain Tumor-Related Epilepsy: A Systematic Review.Brain Sci. 2023 Feb 14;13(2):326. doi: 10.3390/brainsci13020326. Brain Sci. 2023. PMID: 36831869 Free PMC article. Review.
-
Levetiracetam Prophylaxis Therapy for Brain Tumor-Related Epilepsy (BTRE) Is Associated With a Higher Psychiatric Burden.Front Neurol. 2022 Jan 11;12:806839. doi: 10.3389/fneur.2021.806839. eCollection 2021. Front Neurol. 2022. PMID: 35087476 Free PMC article.
-
Perampanel Confirms to Be Effective and Well-Tolerated as an Add-On Treatment in Patients With Brain Tumor-Related Epilepsy (PERADET Study).Front Neurol. 2020 Jun 25;11:592. doi: 10.3389/fneur.2020.00592. eCollection 2020. Front Neurol. 2020. PMID: 32695064 Free PMC article.
-
Effect of Brivaracetam on Efficacy and Tolerability in Patients With Brain Tumor-Related Epilepsy: A Retrospective Multicenter Study.Front Neurol. 2020 Aug 19;11:813. doi: 10.3389/fneur.2020.00813. eCollection 2020. Front Neurol. 2020. PMID: 32973649 Free PMC article.
Cited by
-
Status epilepticus in patients with brain tumors and metastases: A multicenter cohort study of 208 patients and literature review.Neurol Res Pract. 2024 Apr 4;6(1):19. doi: 10.1186/s42466-024-00314-7. Neurol Res Pract. 2024. PMID: 38570823 Free PMC article.
-
Seizure Management and Prophylaxis Considerations in Patients with Brain Tumors.Curr Oncol Rep. 2023 Jul;25(7):787-792. doi: 10.1007/s11912-023-01410-8. Epub 2023 Apr 18. Curr Oncol Rep. 2023. PMID: 37071297 Free PMC article. Review.
-
Temporal PLGG and epilepsy.Childs Nerv Syst. 2024 Oct;40(10):3301-3307. doi: 10.1007/s00381-024-06580-9. Epub 2024 Sep 17. Childs Nerv Syst. 2024. PMID: 39289197 Review.
-
Glioblastoma in the oldest old: Clinical characteristics, therapy, and outcome in patients aged 80 years and older.Neurooncol Pract. 2023 Oct 20;11(2):132-141. doi: 10.1093/nop/npad070. eCollection 2024 Apr. Neurooncol Pract. 2023. PMID: 38496908 Free PMC article.
-
Clinical characteristics and surgical outcomes of low-grade epilepsy-associated brain tumors.Ther Adv Neurol Disord. 2024 Mar 22;17:17562864241237851. doi: 10.1177/17562864241237851. eCollection 2024. Ther Adv Neurol Disord. 2024. PMID: 38525487 Free PMC article.
References
-
- le Rhun E, Guckenberger M, Smits M, Dummer R, Bachelot T, Sahm F, Galldiks N, de Azambuja E, Berghoff AS, Metellus P, Peters S, Hong Y-K, Winkler F, Schadendorf D, van den Bent M, Seoane J, Stahel R, Minniti G, Wesseling P, Weller M, Preusser M. EANO-ESMO clinical practice guidelines for diagnosis, treatment and follow-up of patients with brain metastasis from solid tumours. Annals of Oncology. 2021;32(11):1332–1347. doi: 10.1016/j.annonc.2021.07.016. - DOI - PubMed
-
- Pallud J, Audureau E, Blonski M, Sanai N, Bauchet L, Fontaine D, Mandonnet E, Dezamis E, Psimaras D, Guyotat J, Peruzzi P, Page P, Gal B, Párraga E, Baron M-H, Vlaicu M, Guillevin R, Devaux B, Duffau H, Taillandier L, Capelle L, Huberfeld G. Epileptic seizures in diffuse low-grade gliomas in adults. Brain. 2014;137(2):449–462. doi: 10.1093/brain/awt345. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources