

Role of precipitants in transition of acute decompensation to acute-on-chronic liver failure in patients with HBV-related cirrhosis
- PMID: 36052222
- PMCID: PMC9424579
- DOI: 10.1016/j.jhepr.2022.100529
Role of precipitants in transition of acute decompensation to acute-on-chronic liver failure in patients with HBV-related cirrhosis
Abstract
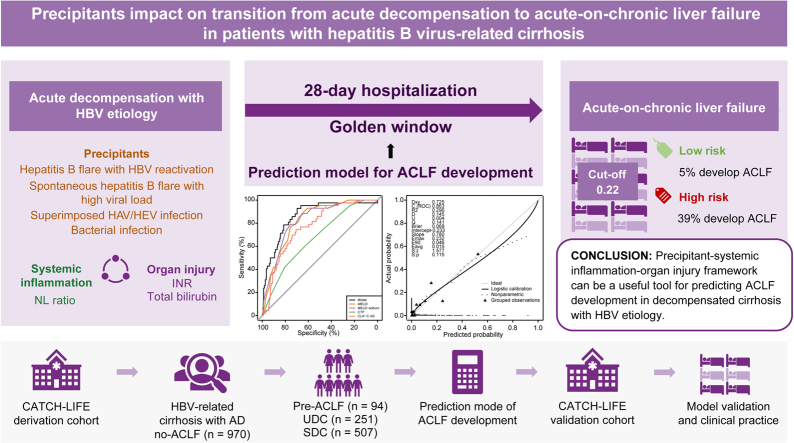
Background & aims: Pre-acute-on-chronic liver failure (ACLF) is a distinct intermediate stage between acute decompensation (AD) and ACLF. However, identifying patients with pre-ACLF and predicting progression from AD to ACLF is difficult. This study aimed to identify pre-ACLF within 28 days, and to develop and validate a prediction model for ACLF in patients with HBV-related decompensated cirrhosis.
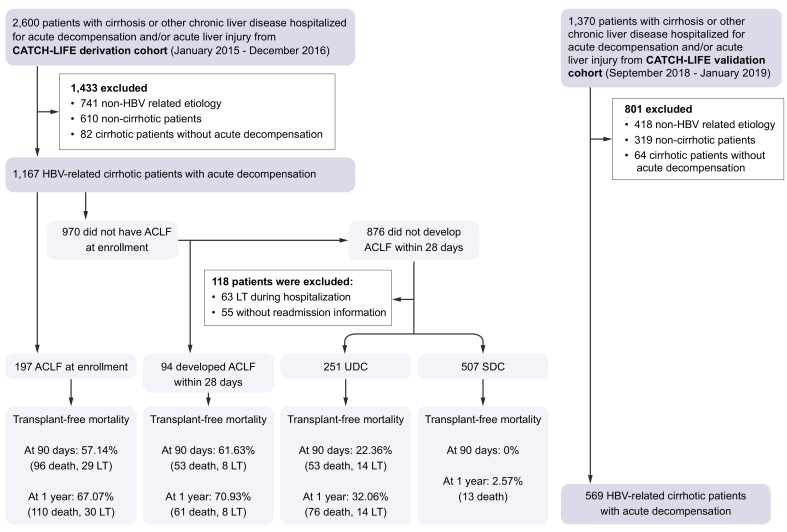
Methods: In total, 1,736 patients with HBV-related cirrhosis and AD were enrolled from 2 large-scale, multicenter, prospective cohorts. ACLF occurrence within 28 days, readmission, and 3-month and 1-year outcomes were collected.
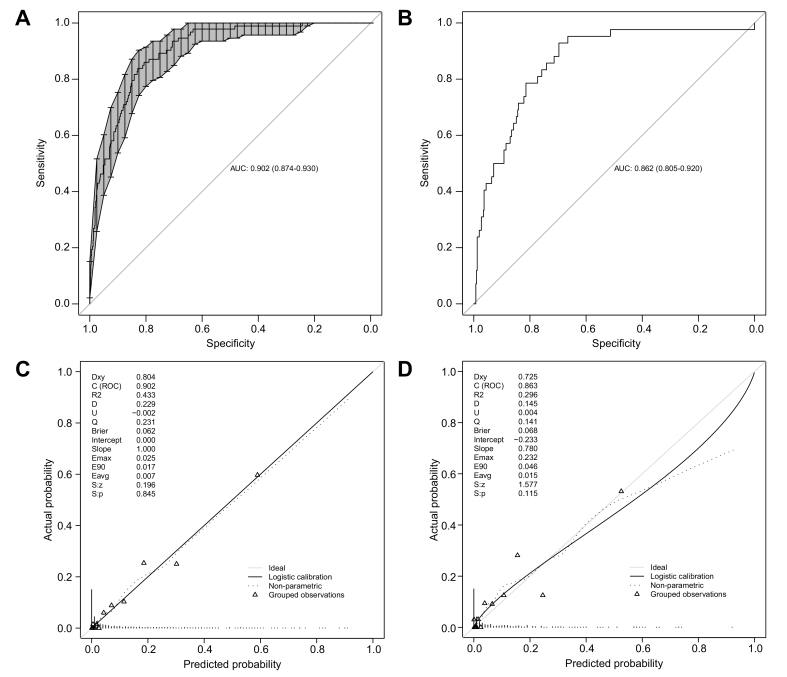
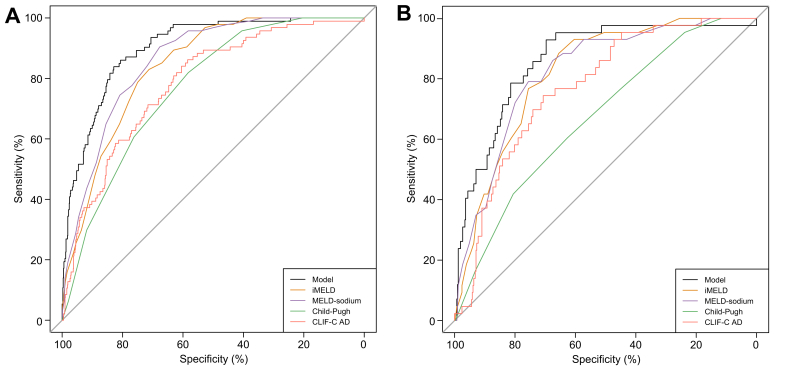
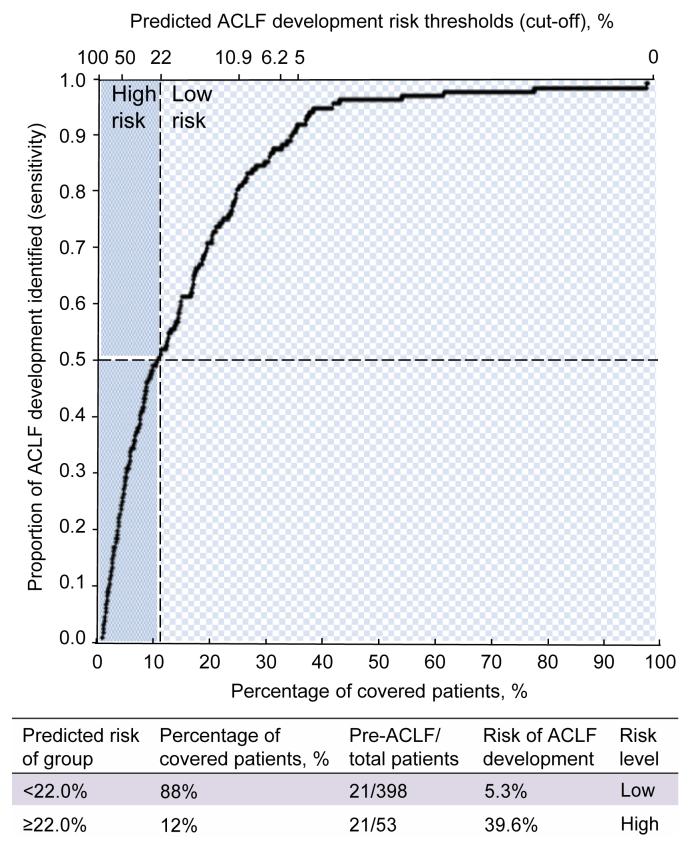
Results: Among 970 patients with AD without ACLF in the derivation cohort, the 94 (9.6%) patients with pre-ACLF had the highest 3-month and 1-year LT-free mortality (61.6% and 70.9%, respectively), which was comparable to those with ACLF at enrollment (57.1% and 67.1%); the 251 (25.9%) patients with unstable decompensated cirrhosis had mortality rates of 22.4% and 32.1%, respectively; while the 507 (57.9%) patients with stable decompensated cirrhosis had the best outcomes (1-year mortality rate of 2.6%). Through Cox proportional hazard regression, specific precipitants, including hepatitis B flare with HBV reactivation, spontaneous hepatitis B flare with high viral load, superimposed infection on HBV, and bacterial infection, were identified to be significantly associated with ACLF occurrence in the derivation cohort. A model that incorporated precipitants, indicators of systemic inflammation and organ injuries reached a high C-index of 0.90 and 0.86 in derivation and validation cohorts, respectively. The optimal cut-off value (0.22) differentiated high-risk and low-risk patients, with a negative predictive value of 0.95.
Conclusions: Three distinct clinical courses of patients with AD are validated in the HBV-etiology population. The precipitants significantly impact on AD-ACLF transition. A model developed by the precipitant-systemic inflammation-organ injury framework could be a useful tool for predicting ACLF occurrence.
Clinical trial number: NCT02457637 and NCT03641872.
Lay summary: It was previously shown that patients with decompensated cirrhosis could be stratified into 3 groups based on their short-term clinical prognoses. Herein, we showed that this stratification applies to patients who develop cirrhosis as a result of hepatitis B virus infection. We also developed a precipitant-based model (i.e. a model that incorporated information about the exact cause of decompensation) that could predict the likelihood of these patients developing a very severe liver disease called acute-on-chronic liver failure (or ACLF).
Keywords: ACLF, acute-on-chronic liver failure; AD, acute decompensation; ALT, alanine aminotransferase; AST, aspartate aminotransferase; CATCH-LIFE study, Chinese AcuTe-On-Chronic LIver FailurE Study; CLIF, Chronic Liver Failure; CLIF-C AD, CLIF consortium acute decompensation score; CRP, C-reactive protein; EASL, European Association for the Study of the Liver; HR, hazard ratio; INR, international normalized ratio; LT, liver transplantation; MELD, model for end-stage liver disease; NL, neutrophil-lymphocyte ratio; NPV, negative predictive value; OFs, organ failures; PPV, positive predictive value; PVT, portal vein thrombosis; SDC, stable decompensated cirrhosis; UDC, unstable decompensated cirrhosis; WBC, white blood cell; acute-on-chronic liver failure; acutely decompensated cirrhosis; hepatitis B virus; iMELD, integrated MELD; precipitants; prediction model.
© 2022 The Author(s).
Conflict of interest statement
The authors declare no conflicts of interest that pertain to this work. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
Comment in
-
A new model for identification of HBV-related pre-ACLF.JHEP Rep. 2022 Aug 17;4(10):100554. doi: 10.1016/j.jhepr.2022.100554. eCollection 2022 Oct. JHEP Rep. 2022. PMID: 36119720 Free PMC article. No abstract available.
Similar articles
-
The PREDICT study uncovers three clinical courses of acutely decompensated cirrhosis that have distinct pathophysiology.J Hepatol. 2020 Oct;73(4):842-854. doi: 10.1016/j.jhep.2020.06.013. Epub 2020 Jul 13. J Hepatol. 2020. PMID: 32673741
-
Transplantation for EASL-CLIF and APASL acute-on-chronic liver failure (ACLF) patients: The TEA cohort to evaluate long-term post-Transplant outcomes.EClinicalMedicine. 2022 Jun 4;49:101476. doi: 10.1016/j.eclinm.2022.101476. eCollection 2022 Jul. EClinicalMedicine. 2022. PMID: 35747194 Free PMC article.
-
PREDICT identifies precipitating events associated with the clinical course of acutely decompensated cirrhosis.J Hepatol. 2021 May;74(5):1097-1108. doi: 10.1016/j.jhep.2020.11.019. Epub 2020 Nov 20. J Hepatol. 2021. PMID: 33227350
-
Acute-on-Chronic Liver Failure: Recent Concepts.J Clin Exp Hepatol. 2015 Mar;5(1):81-5. doi: 10.1016/j.jceh.2014.09.003. Epub 2014 Oct 3. J Clin Exp Hepatol. 2015. PMID: 25941435 Free PMC article. Review.
-
Prognostic assessment of liver cirrhosis and its complications: current concepts and future perspectives.Front Med (Lausanne). 2023 Sep 14;10:1268102. doi: 10.3389/fmed.2023.1268102. eCollection 2023. Front Med (Lausanne). 2023. PMID: 37780566 Free PMC article. Review.
Cited by
-
A new model for identification of HBV-related pre-ACLF.JHEP Rep. 2022 Aug 17;4(10):100554. doi: 10.1016/j.jhepr.2022.100554. eCollection 2022 Oct. JHEP Rep. 2022. PMID: 36119720 Free PMC article. No abstract available.
-
Early prediction of acute-on-chronic liver failure development in patients with diverse chronic liver diseases.Sci Rep. 2024 Nov 15;14(1):28245. doi: 10.1038/s41598-024-79486-w. Sci Rep. 2024. PMID: 39548240 Free PMC article.
-
Intrahepatic macrophage reprogramming associated with lipid metabolism in hepatitis B virus-related acute-on-chronic liver failure.J Transl Med. 2023 Jun 28;21(1):419. doi: 10.1186/s12967-023-04294-1. J Transl Med. 2023. PMID: 37380987 Free PMC article.
-
Prognostic Value of High-Density Lipoprotein Cholesterol in Patients with Overt Hepatic Encephalopathy.Biomedicines. 2024 Aug 6;12(8):1783. doi: 10.3390/biomedicines12081783. Biomedicines. 2024. PMID: 39200247 Free PMC article.
-
Acute decompensation of cirrhosis versus acute-on-chronic liver failure: What are the clinical implications?United European Gastroenterol J. 2024 Mar;12(2):194-202. doi: 10.1002/ueg2.12538. Epub 2024 Feb 20. United European Gastroenterol J. 2024. PMID: 38376886 Free PMC article. Review.
References
-
- Sepanlou S.G., Safiri S., Bisignano C., Ikuta K.S., Merat S., Saberifiroozi M., et al. The global, regional, and national burden of cirrhosis by cause in 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Gastroenterol Hepatol. 2020;5(3):245–266. - PMC - PubMed
-
- Jepsen P., Younossi Z.M. The global burden of cirrhosis: a review of disability-adjusted life-years lost and unmet needs. J Hepatol. 2021;75(Suppl 1):S3–S13. - PubMed
-
- European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J Hepatol. 2018;69(2):406–460. - PubMed
-
- Asrani S.K., Devarbhavi H., Eaton J., Kamath P.S. Burden of liver diseases in the world. J Hepatol. 2019;70(1):151–171. - PubMed
-
- Trebicka J., Fernandez J., Papp M., Caraceni P., Laleman W., Gambino C., et al. The PREDICT study uncovers three clinical courses of acutely decompensated cirrhosis that have distinct pathophysiology. J Hepatol. 2020;73(4):842–854. - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
