

Visceral adipose volume is correlated with surgical tissue fibrosis in Crohn's disease of the small bowel
- PMID: 36042948
- PMCID: PMC9420045
- DOI: 10.1093/gastro/goac044
Visceral adipose volume is correlated with surgical tissue fibrosis in Crohn's disease of the small bowel
Abstract
Background: This study explored the diagnostic performance of visceral adiposity to predict the degree of intestinal inflammation and fibrosis.
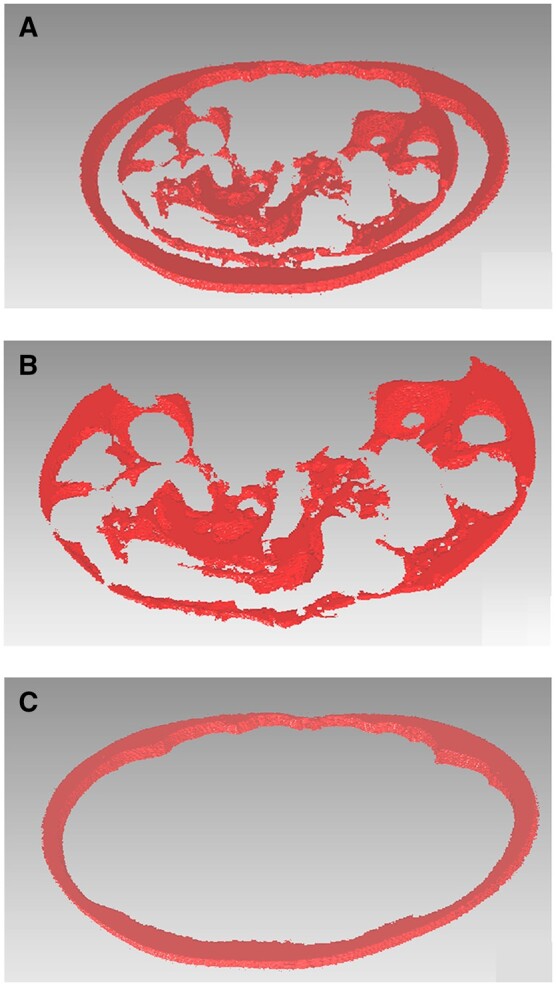
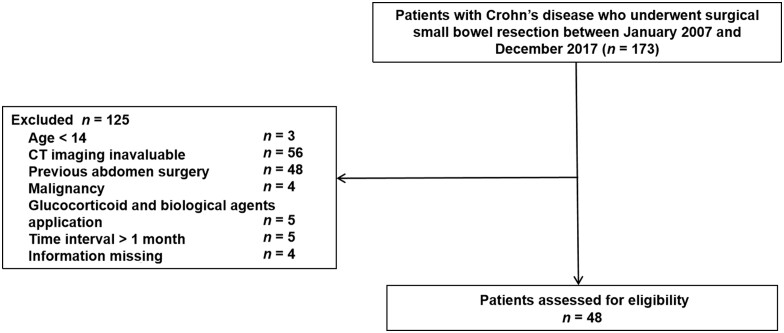
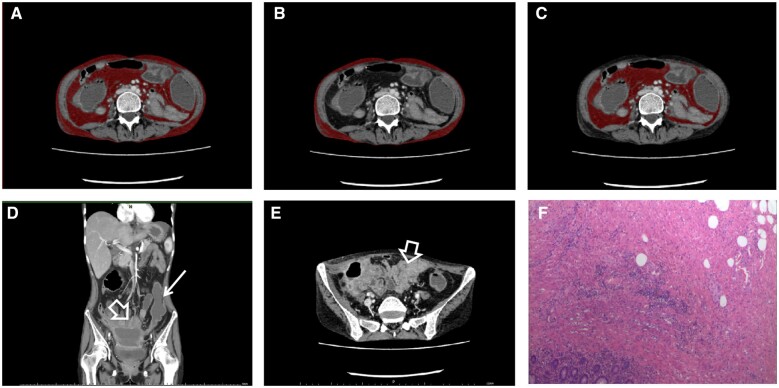
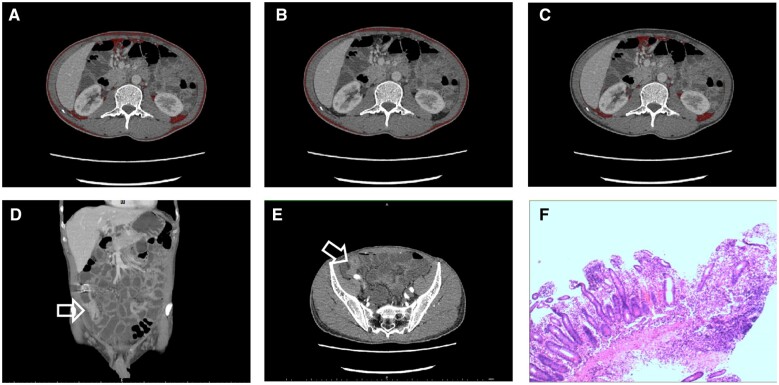
Methods: The patients with Crohn's disease (CD) who underwent surgical small bowel resection at the First Affiliated Hospital of Sun Yat-sen University (Guangzhou, China) between January 2007 and December 2017 were enrolled. We evaluated the intestinal imaging features of computed tomography enterography (CTE), including mesenteric inflammatory fat stranding, the target sign, mesenteric hypervascularity, bowel wall thickening, lymphadenopathy, stricture diameter, and maximal upstream diameter. We used A.K. software (Artificial Intelligence Kit, version 1.1) to calculate the visceral fat (VF) and subcutaneous fat (SF) volumes at the third lumbar vertebra level. Pathological tissue information was recorded. Diagnostic models were established based on the multivariate regression analysis results, and their effectiveness was evaluated by area under the curve (AUC) and decision curve analyses.
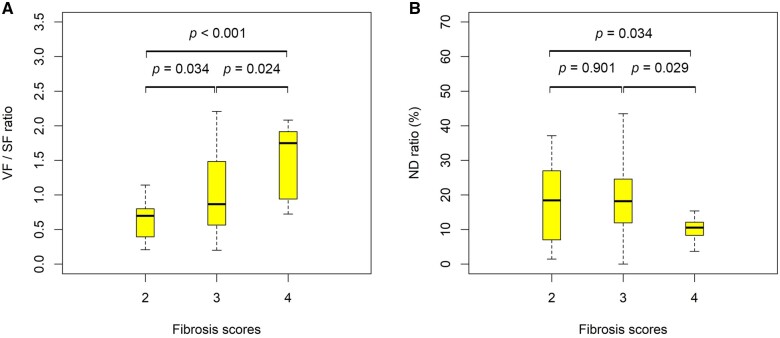
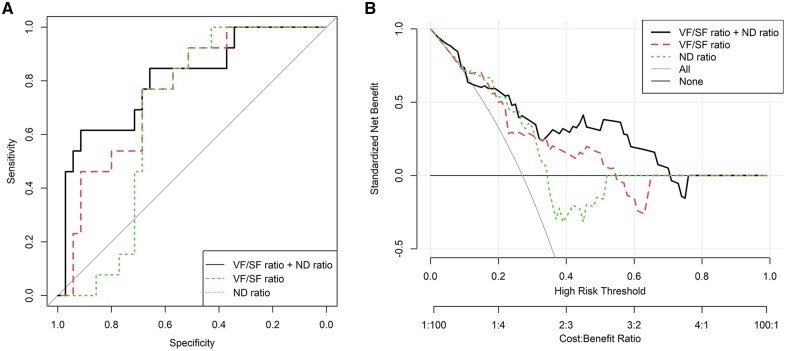
Results: Overall, 48 patients with CD were included in this study. The abdominal VF/SF volume ratio (odds ratio, 1.20; 95% confidence interval, 1.05-1.38; P = 0.009) and the stenosis diameter/upstream intestinal dilatation diameter (ND) ratio (odds ratio, 0.90; 95% confidence interval, 0.82-0.99; P = 0.034) were independent risk factors for the severe fibrosis of the small intestine. The AUC values of the VF/SF ratio, the ND ratio, and their combination were 0.760, 0.673, and 0.804, respectively. The combination of the VS/SF volume ratio and ND ratio achieved the highest net benefit on the decision curve.
Conclusion: The VF volume on CTE can reflect intestinal fibrosis. The combination of the VF/SF volume ratio and ND ratio of CD patients assessed using CTE can help predict severe fibrosis stenosis of the small intestine.
Keywords: Crohn’s disease; computed tomography enterography; intestinal fibrosis; visceral fat.
© The Author(s) 2022. Published by Oxford University Press and Sixth Affiliated Hospital of Sun Yat-sen University.
Figures
Similar articles
-
Visceral adiposity and inflammatory bowel disease.Int J Colorectal Dis. 2021 Nov;36(11):2305-2319. doi: 10.1007/s00384-021-03968-w. Epub 2021 Jun 9. Int J Colorectal Dis. 2021. PMID: 34104989 Review.
-
Computed tomography enterography findings correlate with tissue inflammation, not fibrosis in resected small bowel Crohn's disease.Inflamm Bowel Dis. 2012 May;18(5):849-56. doi: 10.1002/ibd.21801. Epub 2011 Jun 24. Inflamm Bowel Dis. 2012. PMID: 21710535
-
CT-based radiomics signature of visceral adipose tissue for prediction of disease progression in patients with Crohn's disease: A multicentre cohort study.EClinicalMedicine. 2022 Dec 30;56:101805. doi: 10.1016/j.eclinm.2022.101805. eCollection 2023 Feb. EClinicalMedicine. 2022. PMID: 36618894 Free PMC article.
-
Visceral Fat Indices: Do They Help Differentiate Crohn's Disease and Intestinal Tuberculosis in Children?J Crohns Colitis. 2023 Dec 30;17(12):2026-2032. doi: 10.1093/ecco-jcc/jjad109. J Crohns Colitis. 2023. PMID: 37390314
-
Systematic review with meta-analysis: magnetic resonance enterography vs. computed tomography enterography for evaluating disease activity in small bowel Crohn's disease.Aliment Pharmacol Ther. 2014 Jul;40(2):134-46. doi: 10.1111/apt.12815. Epub 2014 Jun 9. Aliment Pharmacol Ther. 2014. PMID: 24912799 Review.
Cited by
-
Enhancing the Differentiation between Intestinal Behçet's Disease and Crohn's Disease through Quantitative Computed Tomography Analysis.Bioengineering (Basel). 2023 Oct 17;10(10):1211. doi: 10.3390/bioengineering10101211. Bioengineering (Basel). 2023. PMID: 37892941 Free PMC article.
-
ELMO1 ameliorates intestinal epithelial cellular senescence via SIRT1/p65 signaling in inflammatory bowel disease-related fibrosis.Gastroenterol Rep (Oxf). 2024 May 14;12:goae045. doi: 10.1093/gastro/goae045. eCollection 2024. Gastroenterol Rep (Oxf). 2024. PMID: 38756351 Free PMC article.
-
Body composition parameters correlate with the endoscopic severity in Crohn's disease patients treated with infliximab.Front Nutr. 2023 Aug 21;10:1251448. doi: 10.3389/fnut.2023.1251448. eCollection 2023. Front Nutr. 2023. PMID: 37674885 Free PMC article.
References
-
- Baumgart DC, Sandborn WJ.. Crohn's disease. Lancet 2012;380:1590–605. - PubMed
-
- Frolkis AD, Dykeman J, Negron ME. et al. Risk of surgery for inflammatory bowel diseases has decreased over time: a systematic review and meta-analysis of population-based studies. Gastroenterology 2013;145:996–1006. - PubMed
LinkOut - more resources
Full Text Sources
