

Mineralocorticoid receptor antagonists and glucocorticoids differentially affect skeletal muscle inflammation and pathology in muscular dystrophy
- PMID: 36040807
- PMCID: PMC9675571
- DOI: 10.1172/jci.insight.159875
Mineralocorticoid receptor antagonists and glucocorticoids differentially affect skeletal muscle inflammation and pathology in muscular dystrophy
Abstract
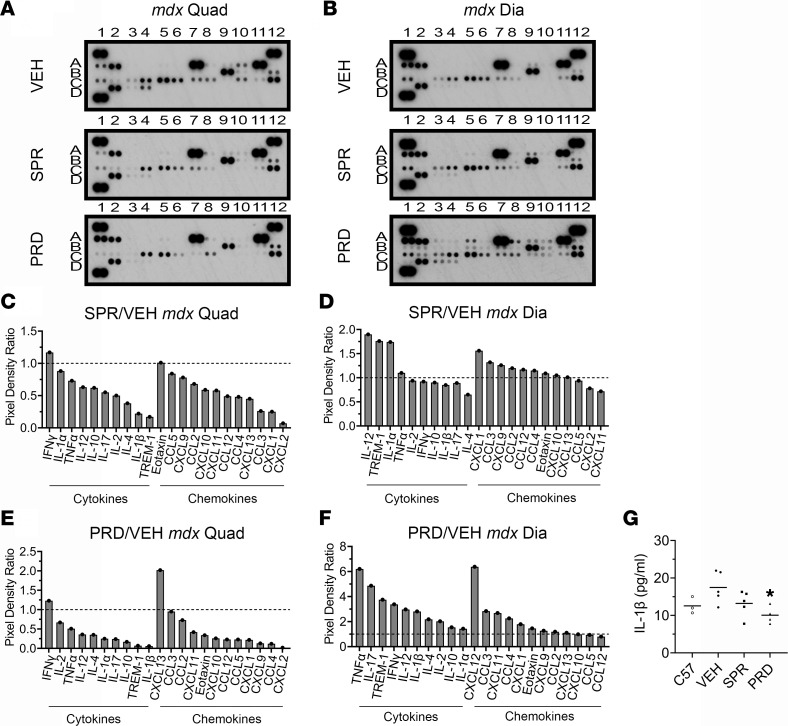
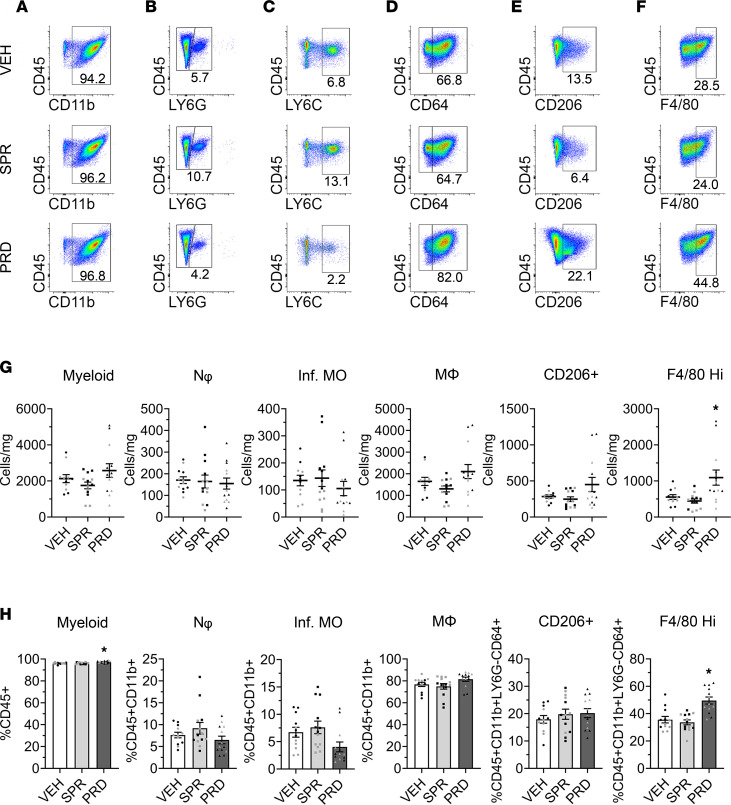
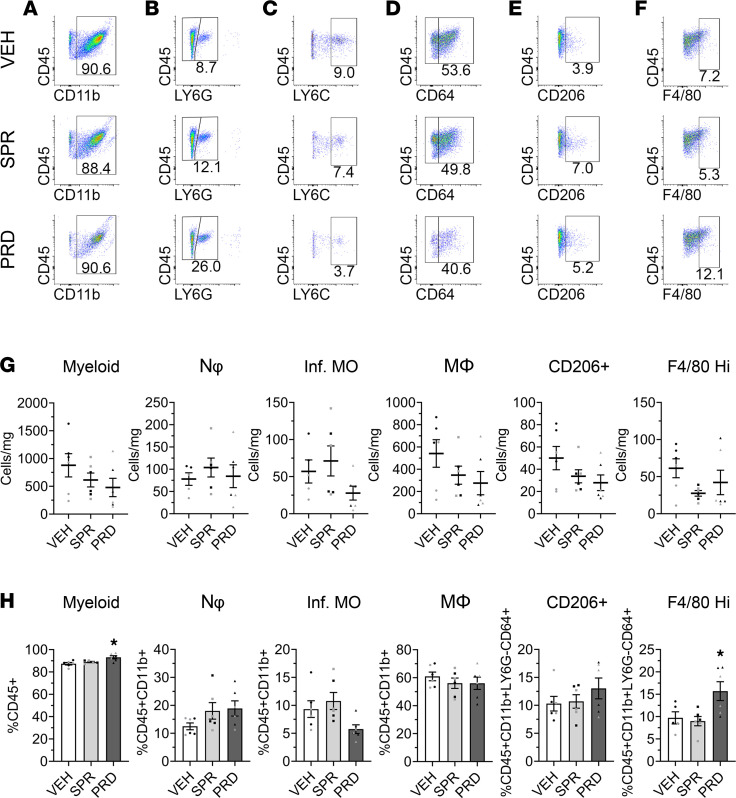
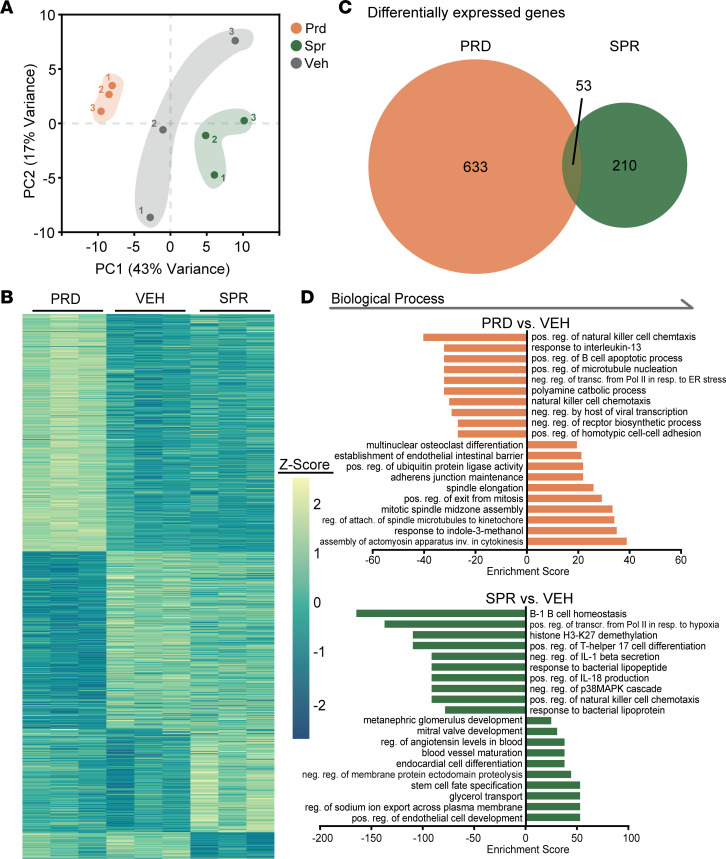
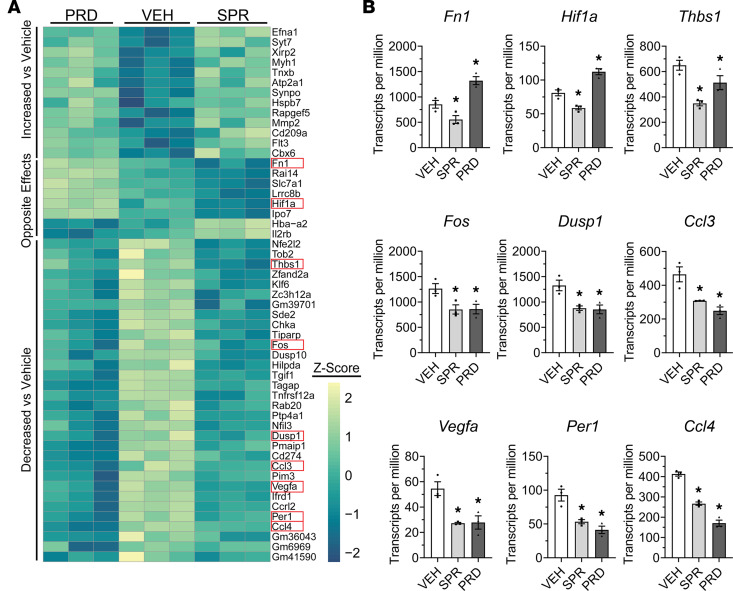
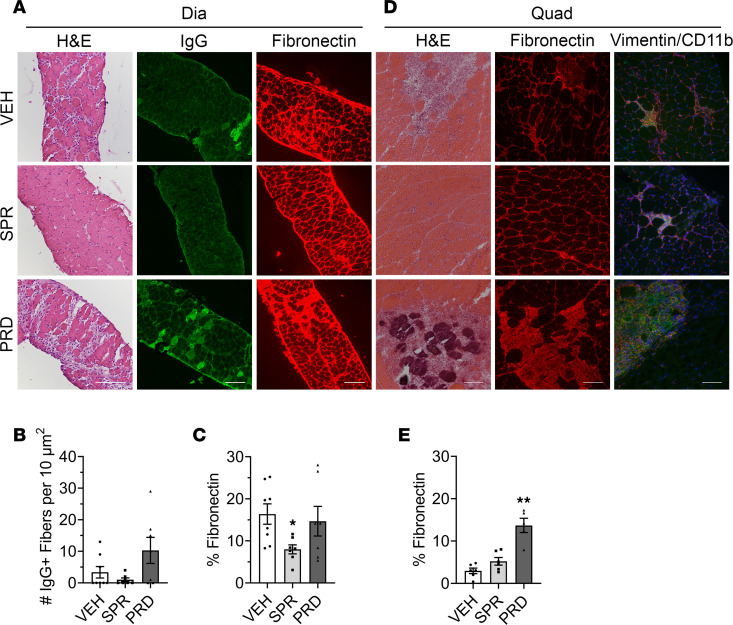
Mineralocorticoid receptor antagonists (MRAs) slow cardiomyopathy in patients with Duchenne muscular dystrophy (DMD) and improve skeletal muscle pathology and function in dystrophic mice. However, glucocorticoids, known antiinflammatory drugs, remain a standard of care for DMD, despite substantial side effects. Exact mechanisms underlying mineralocorticoid receptor (MR) signaling contribution to dystrophy are unknown. Whether MRAs affect inflammation in dystrophic muscles and how they compare with glucocorticoids is unclear. The MRA spironolactone and glucocorticoid prednisolone were each administered for 1 week to dystrophic mdx mice during peak skeletal muscle necrosis to compare effects on inflammation. Both drugs reduced cytokine levels in mdx quadriceps, but prednisolone elevated diaphragm cytokines. Spironolactone did not alter myeloid populations in mdx quadriceps or diaphragms, but prednisolone increased F4/80hi macrophages. Both spironolactone and prednisolone reduced inflammatory gene expression in myeloid cells sorted from mdx quadriceps, while prednisolone additionally perturbed cell cycle genes. Spironolactone also repressed myeloid expression of the gene encoding fibronectin, while prednisolone increased its expression. Overall, spironolactone exhibits antiinflammatory properties without altering leukocyte distribution within skeletal muscles, while prednisolone suppresses quadriceps cytokines but increases diaphragm cytokines and pathology. Antiinflammatory properties of MRAs and different limb and respiratory muscle responses to glucocorticoids should be considered when optimizing treatments for patients with DMD.
Keywords: Cytokines; Innate immunity; Muscle Biology; Skeletal muscle.
Conflict of interest statement
Figures
Similar articles
-
Mineralocorticoid Receptor Antagonists in Muscular Dystrophy Mice During Aging and Exercise.J Neuromuscul Dis. 2018;5(3):295-306. doi: 10.3233/JND-180323. J Neuromuscul Dis. 2018. PMID: 30010143 Free PMC article.
-
Myeloid mineralocorticoid receptors contribute to skeletal muscle repair in muscular dystrophy and acute muscle injury.Am J Physiol Cell Physiol. 2022 Mar 1;322(3):C354-C369. doi: 10.1152/ajpcell.00411.2021. Epub 2022 Jan 19. Am J Physiol Cell Physiol. 2022. PMID: 35044859 Free PMC article.
-
Gene expression effects of glucocorticoid and mineralocorticoid receptor agonists and antagonists on normal human skeletal muscle.Physiol Genomics. 2017 Jun 1;49(6):277-286. doi: 10.1152/physiolgenomics.00128.2016. Epub 2017 Apr 21. Physiol Genomics. 2017. PMID: 28432191 Free PMC article.
-
Mineralocorticoid Receptor Signaling in the Inflammatory Skeletal Muscle Microenvironments of Muscular Dystrophy and Acute Injury.Front Pharmacol. 2022 Jun 28;13:942660. doi: 10.3389/fphar.2022.942660. eCollection 2022. Front Pharmacol. 2022. PMID: 35837290 Free PMC article. Review.
-
Microbes, metabolites and muscle: Is the gut-muscle axis a plausible therapeutic target in Duchenne muscular dystrophy?Exp Physiol. 2023 Sep;108(9):1132-1143. doi: 10.1113/EP091063. Epub 2023 Jun 3. Exp Physiol. 2023. PMID: 37269541 Free PMC article. Review.
Cited by
-
Troponin I Tyrosine Phosphorylation Beneficially Accelerates Diastolic Function.Circ Res. 2024 Jan 5;134(1):33-45. doi: 10.1161/CIRCRESAHA.123.323132. Epub 2023 Dec 14. Circ Res. 2024. PMID: 38095088 Free PMC article.
-
Effect of 11-Deoxycorticosterone in the Transcriptomic Response to Stress in Rainbow Trout Skeletal Muscle.Genes (Basel). 2023 Feb 17;14(2):512. doi: 10.3390/genes14020512. Genes (Basel). 2023. PMID: 36833439 Free PMC article.
-
CB2 Receptor as Emerging Anti-Inflammatory Target in Duchenne Muscular Dystrophy.Int J Mol Sci. 2023 Feb 7;24(4):3345. doi: 10.3390/ijms24043345. Int J Mol Sci. 2023. PMID: 36834757 Free PMC article.
-
The glucocorticoid receptor acts locally to protect dystrophic muscle and heart during disease.Dis Model Mech. 2024 May 1;17(5):dmm050397. doi: 10.1242/dmm.050397. Epub 2024 May 21. Dis Model Mech. 2024. PMID: 38770680 Free PMC article.
-
Cell-type specific effects of mineralocorticoid receptor gene expression suggest intercellular communication regulating fibrosis in skeletal muscle disease.Front Physiol. 2024 Apr 26;15:1322729. doi: 10.3389/fphys.2024.1322729. eCollection 2024. Front Physiol. 2024. PMID: 38737833 Free PMC article.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
