

Pitfalls of Antiretroviral Therapy: Current Status and Long-Term CNS Toxicity
- PMID: 35883450
- PMCID: PMC9312798
- DOI: 10.3390/biom12070894
Pitfalls of Antiretroviral Therapy: Current Status and Long-Term CNS Toxicity
Abstract
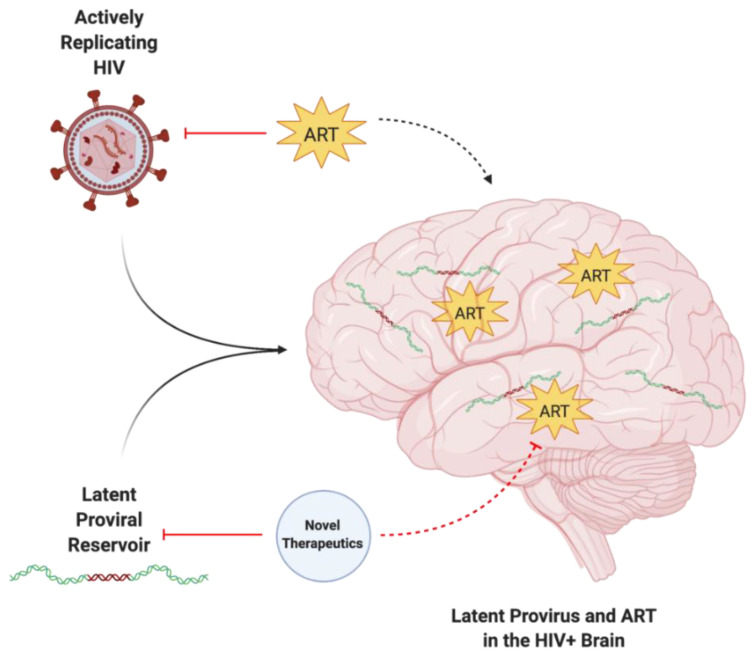
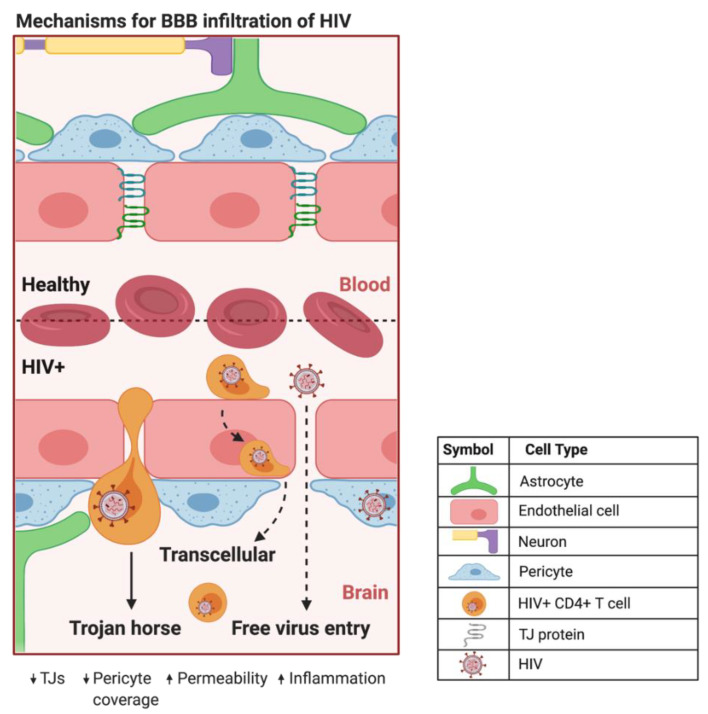
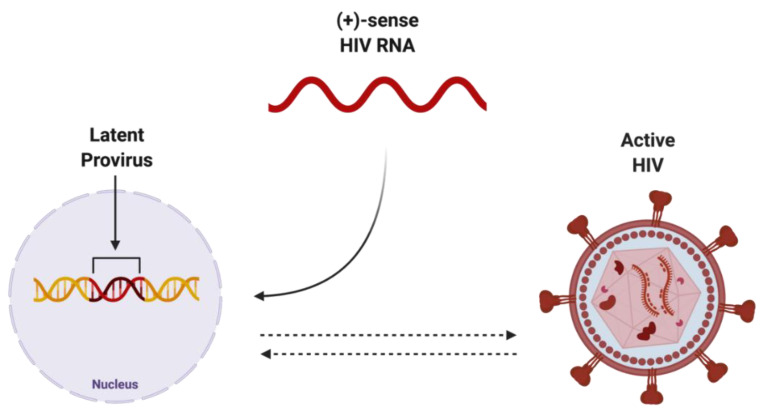
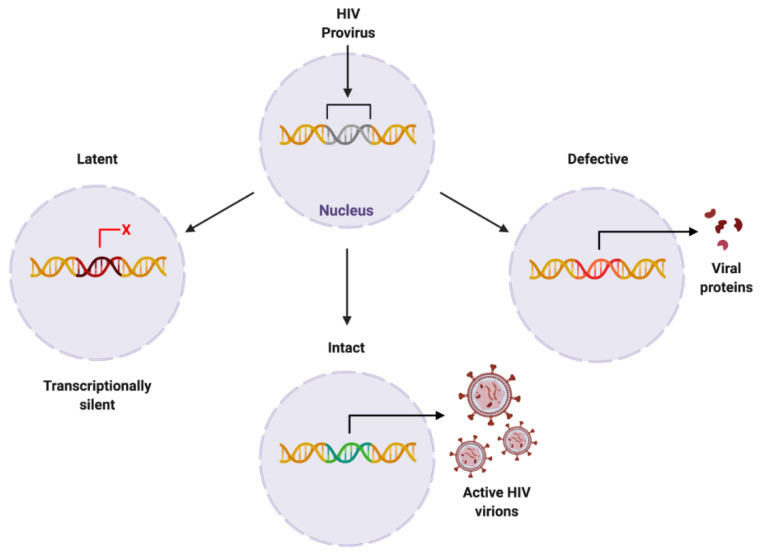
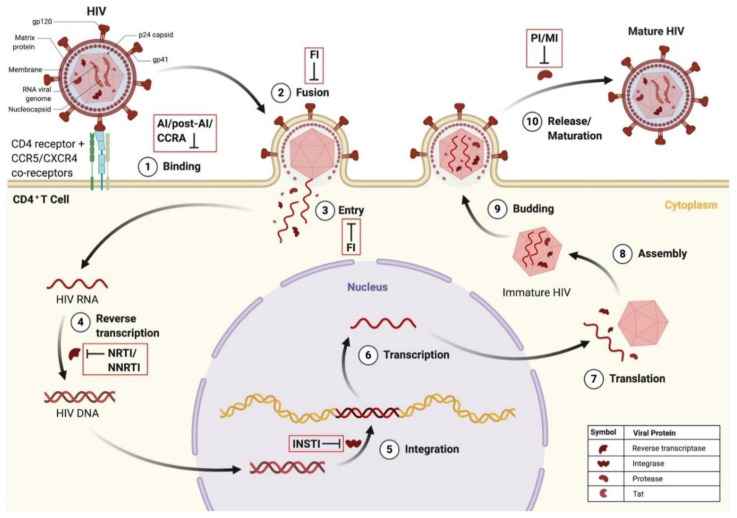
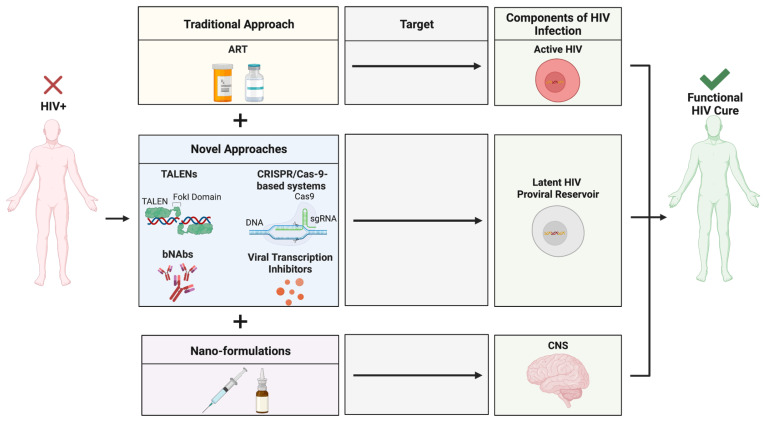
HIV can traverse the BBB using a Trojan horse-like mechanism. Hidden within infected immune cells, HIV can infiltrate the highly safeguarded CNS and propagate disease. Once integrated within the host genome, HIV becomes a stable provirus, which can remain dormant, evade detection by the immune system or antiretroviral therapy (ART), and result in rebound viraemia. As ART targets actively replicating HIV, has low BBB penetrance, and exposes patients to long-term toxicity, further investigation into novel therapeutic approaches is required. Viral proteins can be produced by latent HIV, which may play a synergistic role alongside ART in promoting neuroinflammatory pathophysiology. It is believed that the ability to specifically target these proviral reservoirs would be a vital driving force towards a cure for HIV infection. A novel drug design platform, using the in-tandem administration of several therapeutic approaches, can be used to precisely target the various components of HIV infection, ultimately leading to the eradication of active and latent HIV and a functional cure for HIV. The aim of this review is to explore the pitfalls of ART and potential novel therapeutic alternatives.
Keywords: HIV; antiretroviral therapy; blood-brain barrier; brain; neuroHIV.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
HIV-1 Latency and Viral Reservoirs: Existing Reversal Approaches and Potential Technologies, Targets, and Pathways Involved in HIV Latency Studies.Cells. 2021 Feb 23;10(2):475. doi: 10.3390/cells10020475. Cells. 2021. PMID: 33672138 Free PMC article. Review.
-
HIV type-1 latency: targeted induction of proviral reservoirs.Antivir Chem Chemother. 2009;19(5):177-87. doi: 10.1177/095632020901900501. Antivir Chem Chemother. 2009. PMID: 19483266 Review.
-
Posttranscriptional Regulation of HIV-1 Gene Expression during Replication and Reactivation from Latency by Nuclear Matrix Protein MATR3.mBio. 2018 Nov 13;9(6):e02158-18. doi: 10.1128/mBio.02158-18. mBio. 2018. PMID: 30425153 Free PMC article.
-
A Review of Current Strategies Towards the Elimination of Latent HIV-1 and Subsequent HIV-1 Cure.Curr HIV Res. 2021;19(1):14-26. doi: 10.2174/1570162X18999200819172009. Curr HIV Res. 2021. PMID: 32819259 Free PMC article.
-
Microglial Cells: The Main HIV-1 Reservoir in the Brain.Front Cell Infect Microbiol. 2019 Oct 24;9:362. doi: 10.3389/fcimb.2019.00362. eCollection 2019. Front Cell Infect Microbiol. 2019. PMID: 31709195 Free PMC article. Review.
Cited by
-
Cocaine regulates antiretroviral therapy CNS access through pregnane-x receptor-mediated drug transporter and metabolizing enzyme modulation at the blood brain barrier.Fluids Barriers CNS. 2024 Jan 10;21(1):5. doi: 10.1186/s12987-023-00507-3. Fluids Barriers CNS. 2024. PMID: 38200564 Free PMC article.
-
Adult Human Brain Tissue Cultures to Study NeuroHIV.Cells. 2024 Jun 29;13(13):1127. doi: 10.3390/cells13131127. Cells. 2024. PMID: 38994979 Free PMC article.
-
Chronic brain damage in HIV-infected individuals under antiretroviral therapy is associated with viral reservoirs, sulfatide release, and compromised cell-to-cell communication.Cell Mol Life Sci. 2023 Apr 4;80(4):116. doi: 10.1007/s00018-023-04757-0. Cell Mol Life Sci. 2023. PMID: 37016051 Free PMC article.
-
Perinatal exposure to atazanavir-based antiretroviral regimens in a mouse model leads to differential long-term motor and cognitive deficits dependent on the NRTI backbone.Front Mol Neurosci. 2024 Apr 5;17:1376681. doi: 10.3389/fnmol.2024.1376681. eCollection 2024. Front Mol Neurosci. 2024. PMID: 38646101 Free PMC article.
References
-
- Centers for Disease Control and Prevention HIV Suveillance Report. [(accessed on 19 September 2019)];2018 Available online: http://www.cdc.gov/hiv/library/reports/hiv-surveillance.html.
-
- Akay C., Cooper M., Odeleye A., Jensen B.K., White M.G., Vassoler F., Gannon P.J., Mankowski J., Dorsey J.L., Buch A.M., et al. Antiretroviral drugs induce oxidative stress and neuronal damage in the Central Nervous System. J. NeuroVirology. 2014;20:39–53. doi: 10.1007/s13365-013-0227-1. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
