

Secondary Brain Injury Following Neonatal Intraventricular Hemorrhage: The Role of the Ciliated Ependyma
- PMID: 35844746
- PMCID: PMC9280684
- DOI: 10.3389/fped.2022.887606
Secondary Brain Injury Following Neonatal Intraventricular Hemorrhage: The Role of the Ciliated Ependyma
Abstract
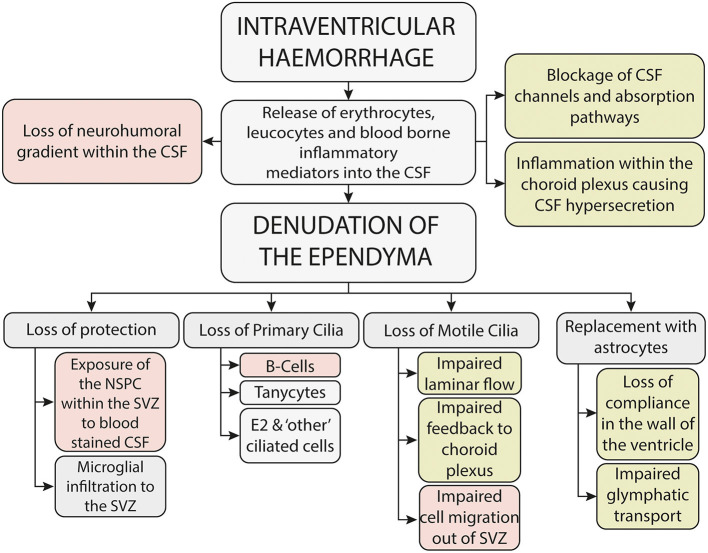
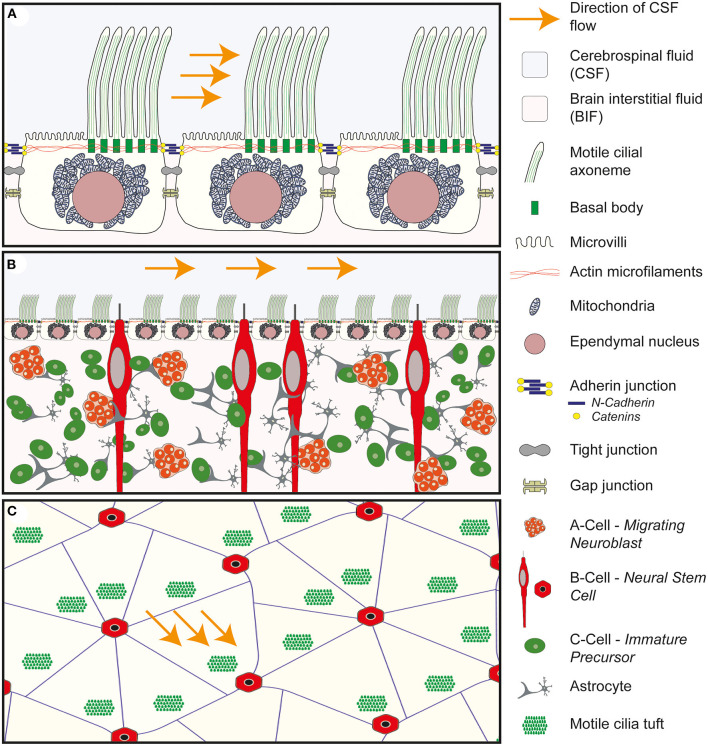
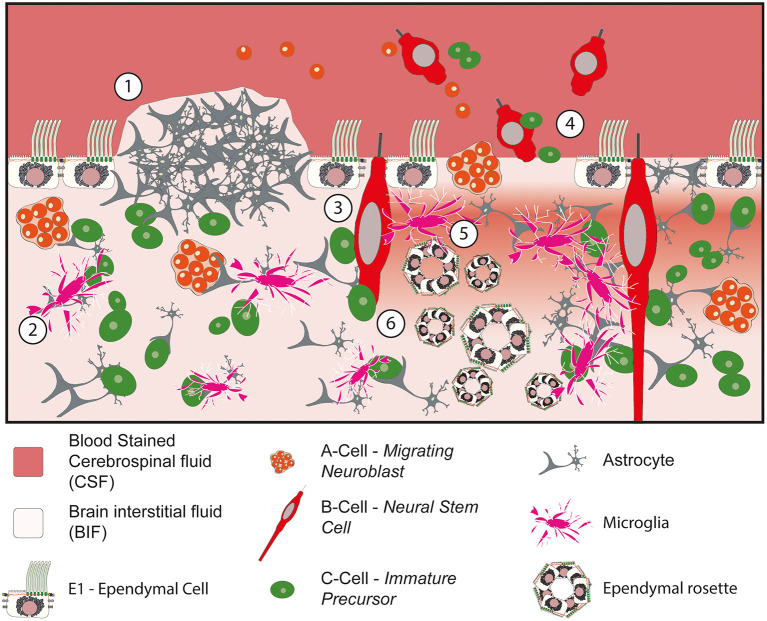
Intraventricular hemorrhage is recognized as a leading cause of hydrocephalus in the developed world and a key determinant of neurodevelopmental outcome following premature birth. Even in the absence of haemorrhagic infarction or posthaemorrhagic hydrocephalus, there is increasing evidence of neuropsychiatric and neurodevelopmental sequelae. The pathophysiology underlying this injury is thought to be due to a primary destructive and secondary developmental insult, but the exact mechanisms remain elusive and this has resulted in a paucity of therapeutic interventions. The presence of blood within the cerebrospinal fluid results in the loss of the delicate neurohumoral gradient within the developing brain, adversely impacting on the tightly regulated temporal and spatial control of cell proliferation and migration of the neural stem progenitor cells within the subventricular zone. In addition, haemolysis of the erythrocytes, associated with the release of clotting factors and leucocytes into the cerebrospinal (CSF), results in a toxic and inflammatory CSF microenvironment which is harmful to the periventricular tissues, resulting in damage and denudation of the multiciliated ependymal cells which line the choroid plexus and ventricular system. The ependyma plays a critical role in the developing brain and beyond, acting as both a protector and gatekeeper to the underlying parenchyma, controlling influx and efflux across the CSF to brain interstitial fluid interface. In this review I explore the hypothesis that damage and denudation of the ependymal layer at this critical juncture in the developing brain, seen following IVH, may adversely impact on the brain microenvironment, exposing the underlying periventricular tissues to toxic and inflammatory CSF, further exacerbating disordered activity within the subventricular zone (SVZ). By understanding the impact that intraventricular hemorrhage has on the microenvironment within the CSF, and the consequences that this has on the multiciliated ependymal cells which line the neuraxis, we can begin to develop and test novel therapeutic interventions to mitigate damage and reduce the associated morbidity.
Keywords: cerebrospinal fluid; ependymal cilia; intraventricular hemorrhage; post haemorrhagic hydrocephalus; subventricular zone (SVZ).
Copyright © 2022 Dawes.
Conflict of interest statement
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
High-Speed Video Microscopy of Ependymal Cilia in Brain Organotypic and Cell Culture Models.Methods Mol Biol. 2024;2725:239-250. doi: 10.1007/978-1-0716-3507-0_15. Methods Mol Biol. 2024. PMID: 37856029
-
Neuroblast proliferation on the surface of the adult rat striatal wall after focal ependymal loss by intracerebroventricular injection of neuraminidase.J Comp Neurol. 2008 Apr 1;507(4):1571-87. doi: 10.1002/cne.21618. J Comp Neurol. 2008. PMID: 18236450
-
Ventricular Zone Disruption in Human Neonates With Intraventricular Hemorrhage.J Neuropathol Exp Neurol. 2017 May 1;76(5):358-375. doi: 10.1093/jnen/nlx017. J Neuropathol Exp Neurol. 2017. PMID: 28521038 Free PMC article.
-
Exploring mechanisms of ventricular enlargement in idiopathic normal pressure hydrocephalus: a role of cerebrospinal fluid dynamics and motile cilia.Fluids Barriers CNS. 2021 Apr 19;18(1):20. doi: 10.1186/s12987-021-00243-6. Fluids Barriers CNS. 2021. PMID: 33874972 Free PMC article. Review.
-
Multiciliated ependymal cells: an update on biology and pathology in the adult brain.Acta Neuropathol. 2024 Sep 10;148(1):39. doi: 10.1007/s00401-024-02784-0. Acta Neuropathol. 2024. PMID: 39254862 Review.
Cited by
-
High-Speed Video Microscopy of Ependymal Cilia in Brain Organotypic and Cell Culture Models.Methods Mol Biol. 2024;2725:239-250. doi: 10.1007/978-1-0716-3507-0_15. Methods Mol Biol. 2024. PMID: 37856029
-
Extrauterine support of pre-term lambs achieves similar transcriptomic profiling to late pre-term lamb brains.Sci Rep. 2024 Nov 21;14(1):28840. doi: 10.1038/s41598-024-79095-7. Sci Rep. 2024. PMID: 39572605 Free PMC article.
-
The Role of Oxidative Stress in the Progression of Secondary Brain Injury Following Germinal Matrix Hemorrhage.Transl Stroke Res. 2024 Jun;15(3):647-658. doi: 10.1007/s12975-023-01147-3. Epub 2023 Mar 17. Transl Stroke Res. 2024. PMID: 36930383 Review.
-
Iron homeostasis and post-hemorrhagic hydrocephalus: a review.Front Neurol. 2024 Jan 12;14:1287559. doi: 10.3389/fneur.2023.1287559. eCollection 2023. Front Neurol. 2024. PMID: 38283681 Free PMC article. Review.
-
Therapeutic strategies to recover ependymal barrier after inflammatory damage: relevance for recovering neurogenesis during development.Front Neurosci. 2023 Jun 15;17:1204197. doi: 10.3389/fnins.2023.1204197. eCollection 2023. Front Neurosci. 2023. PMID: 37397456 Free PMC article. Review.
References
Publication types
LinkOut - more resources
Full Text Sources