

Positron emission tomography/computed tomography and endobronchial ultrasound-guided transbronchial needle aspiration to evaluate the status of N2 in preoperative non-small cell lung cancer: a diagnostic test
- PMID: 35813743
- PMCID: PMC9264044
- DOI: 10.21037/jtd-22-521
Positron emission tomography/computed tomography and endobronchial ultrasound-guided transbronchial needle aspiration to evaluate the status of N2 in preoperative non-small cell lung cancer: a diagnostic test
Abstract
Background: As a minimally invasive method, endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) was more accurate than non-invasive methods such as positron emission tomography (PET) and computed tomography (CT) to evaluate the lymph nodes in preoperative non-small cell lung cancer (NSCLC). PET/CT has more anatomical advantages than PET scanning and is more accurate in lung cancer staging. However, no relevant studies have comparatively evaluated PET/CT and EBUS-TBNA for NSCLC patients.
Methods: A total of 112 patients were included in this retrospective analysis. The golden diagnosis of N2 status was postoperative pathological results. In EBUS-TBNA puncture specimens, if clear malignant tumor cells could be seen, the results were taken as positive. In PET/CT image analysis, the CT values, short diameter, and maximum standardized uptake value (SUVmax) of each lymph node were recorded to evaluate N2 status. The results of PET/CT and EBUS-TBNA were compared with the final pathological results, and respective sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy were calculated. - Then, the patients were divided into adenocarcinoma group and squamous cell carcinoma group -and the results were calculated and compared with the above method.
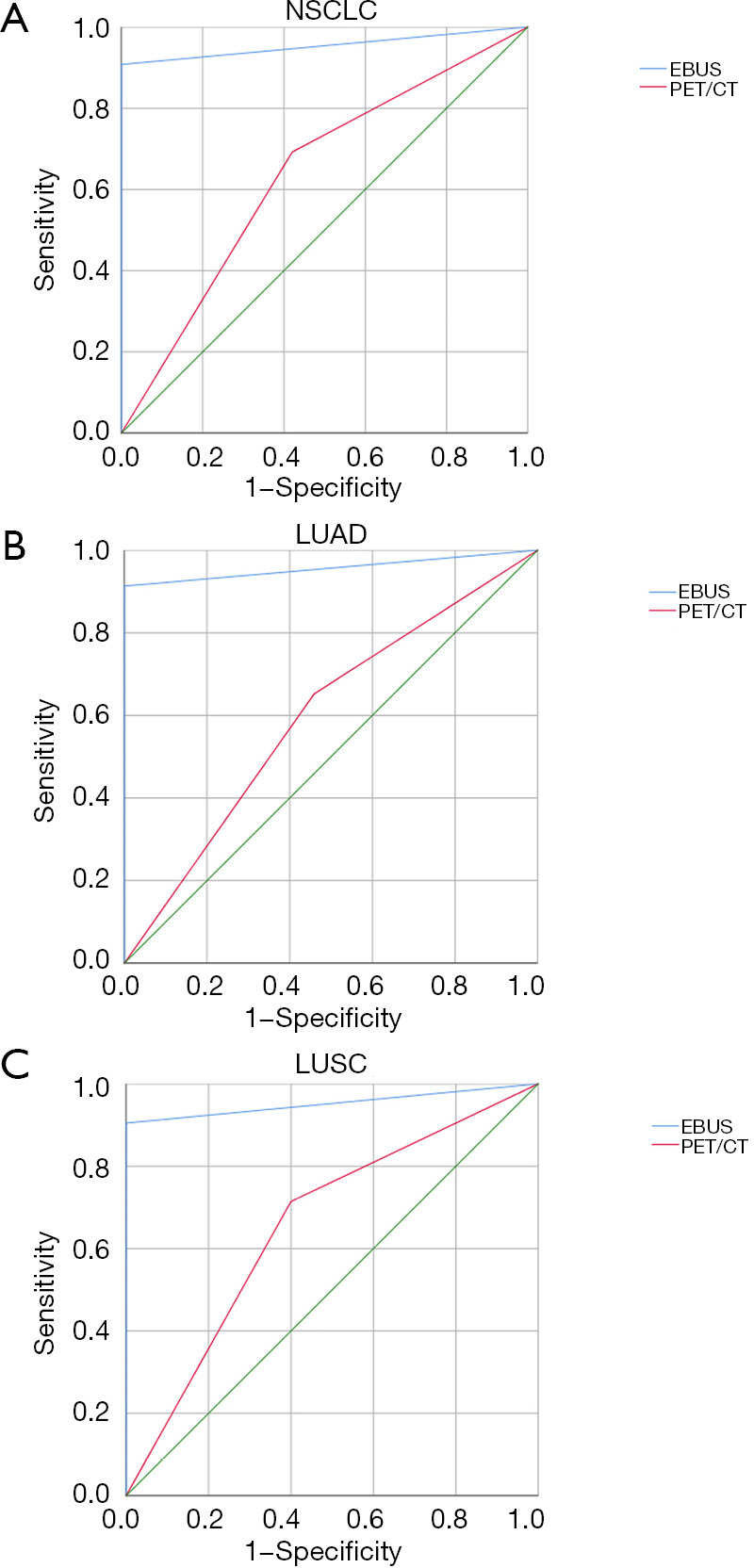
Results: The results showed that EBUS-TBNA had a higher diagnostic value for mediastinal lymph nodes than PET/CT, and the difference was statistically significant (P<0.001). In NSCLC patients, the results showed that the sensitivity (P=0.013), specificity (P<0.001), PPV (P<0.001), NPV (P<0.001), and accuracy (P<0.001) of EBUS-TBNA were higher than that of PET/CT (AUC =0.954 and 0.636, respectively). In adenocarcinoma cases, specificity (P<0.001), PPV (P<0.001), NPV (P<0.001), and accuracy (P<0.001) of EBUS-TBNA were higher than that of PET/CT (AUC =0.957 and 0.596, respectively).In cases with squamous cell carcinoma, specificity (P=0.003), PPV (P<0.001), and accuracy (P<0.001) of EBUS-TBNA were higher than PET/CT (AUC =0.952 and 0.657, respectively).
Conclusions: For preoperative diagnosis of mediastinal lymph node metastases in NSCLC, EBUS-TBNA is more accurate than PET/CT. For those patients with suspected mediastinal lymph node metastasis, EBUS-TBNA should be preferred method to evaluate the status of mediastinal lymph nodes.
Keywords: Non-small cell lung cancer (NSCLC); endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA); mediastinal lymph node staging; positron emission tomography/computed tomography (PET/CT).
2022 Journal of Thoracic Disease. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://jtd.amegroups.com/article/view/10.21037/jtd-22-521/coif). The authors have no conflicts of interest to declare.
Figures
Similar articles
-
Impact of 18F-FDG PET/CT, CT and EBUS/TBNA on preoperative mediastinal nodal staging of NSCLC.BMC Med Imaging. 2021 Mar 17;21(1):49. doi: 10.1186/s12880-021-00580-w. BMC Med Imaging. 2021. PMID: 33731050 Free PMC article.
-
Application of endobronchial ultrasound-guided transbronchial needle aspiration following integrated PET/CT in mediastinal staging of potentially operable non-small cell lung cancer.Chest. 2009 May;135(5):1280-1287. doi: 10.1378/chest.08-2019. Epub 2008 Dec 31. Chest. 2009. PMID: 19118267
-
EBUS-TBNA for mediastinal staging of centrally located T1N0M0 non-small cell lung cancer clinically staged with PET/CT.Respirology. 2024 Feb;29(2):158-165. doi: 10.1111/resp.14613. Epub 2023 Oct 27. Respirology. 2024. PMID: 37885329
-
Mediastinal staging for non-small cell lung cancer.Transl Lung Cancer Res. 2021 Jan;10(1):496-505. doi: 10.21037/tlcr.2020.03.08. Transl Lung Cancer Res. 2021. PMID: 33569331 Free PMC article. Review.
-
Endobronchial ultrasound-guided transbronchial mediastinal cryobiopsy: a narrative review.Mediastinum. 2023 Dec 4;8:2. doi: 10.21037/med-23-34. eCollection 2024. Mediastinum. 2023. PMID: 38322189 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources
Research Materials