

Physiologic Transdermal Estradiol Replacement Mimics Effects of Endogenous Estrogen on Bone Outcomes in Hypoestrogenic Women with Anorexia Nervosa
- PMID: 35807738
- PMCID: PMC9268216
- DOI: 10.3390/nu14132557
Physiologic Transdermal Estradiol Replacement Mimics Effects of Endogenous Estrogen on Bone Outcomes in Hypoestrogenic Women with Anorexia Nervosa
Abstract
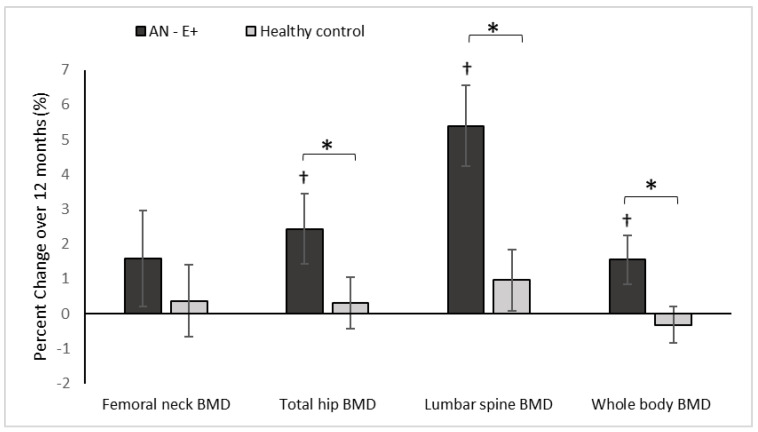
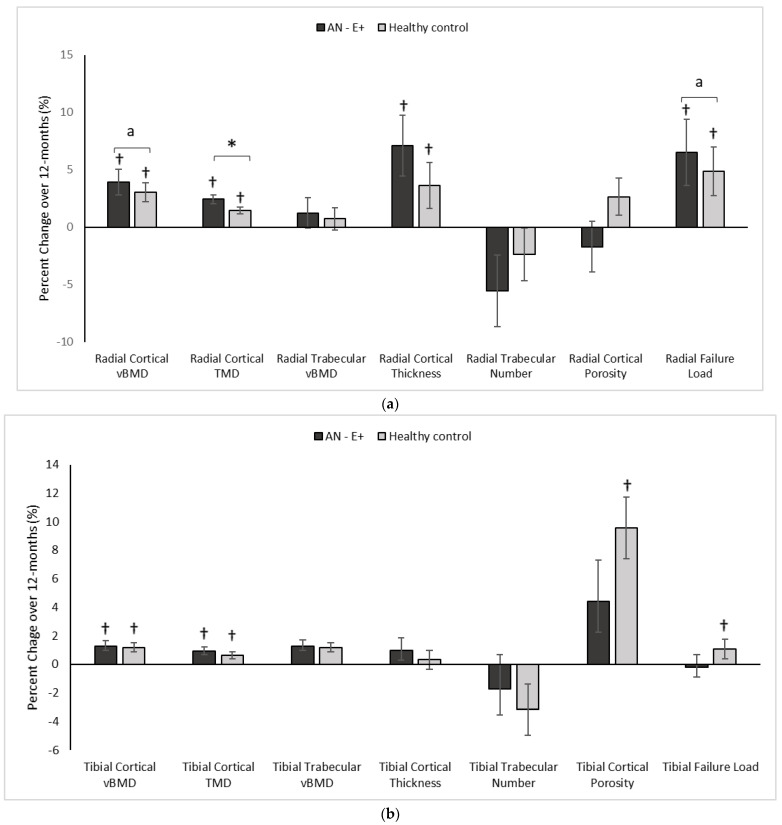
Background: While physiologic estrogen replacement results in increases in areal bone mineral density (aBMD) in hypoestrogenic adolescent girls and young adult women with AN, data are lacking regarding its impact on measures of volumetric BMD (vBMD), bone geometry, and structure. Methods: 23 young women with anorexia nervosa (AN) and 27 normal-weight healthy controls (HC) between 14−25 years old were followed for 12 months. AN participants received transdermal 17β-estradiol (continuously) with 10 days of cyclic oral progesterone (100 mg daily) every month for the study duration (AN-E+). DXA was used to measure aBMD and body composition, high resolution peripheral quantitative CT (HRpQCT) to assess vBMD, bone geometry and structure at the distal radius and tibia, and microfinite element analysis to estimate strength. Results: Groups did not differ for age. Median baseline BMI z-scores were −1.13 (−1.58, −0.38) in AN-E+ vs. 0.08 (−0.40, 0.84) in HC (p < 0.0001). For most HRpQCT parameters and strength estimates, young women with AN receiving physiologic estrogen replacement demonstrated similar changes over 12 months as did normoestrogenic HC. Additionally, radial cortical tissue mineral density, cortical vBMD, and failure load increased (p = 0.01; p = 0.02; p = 0.004 respectively) over 12 months in AN-E+ compared to HC. Conclusions: With physiologic estrogen replacement, bone accrual improved in AN to approximate changes observed in normoestrogenic controls followed without any intervention, with additional benefits observed for cortical tissue mineral density, cortical vBMD, and failure load at the radius in AN vs. controls. Thus, this strategy for estrogen replacement effectively mimics the effects of endogenous estrogen on bone structure and estimated strength.
Keywords: adolescents; anorexia nervosa; bone density; bone structure; estradiol.
Conflict of interest statement
M.M. has served as a consultant for Abbvie and Sanofi and on the Scientific Advisory Board of Abbvie and Ipsen. All other authors declare no conflict of interest.
Figures
Similar articles
-
Suboptimal bone microarchitecure in adolescent girls with obesity compared to normal-weight controls and girls with anorexia nervosa.Bone. 2019 May;122:246-253. doi: 10.1016/j.bone.2019.03.007. Epub 2019 Mar 7. Bone. 2019. PMID: 30853658 Free PMC article.
-
Effect of Transdermal Estradiol and Insulin-like Growth Factor-1 on Bone Endpoints of Young Women With Anorexia Nervosa.J Clin Endocrinol Metab. 2021 Jun 16;106(7):2021-2035. doi: 10.1210/clinem/dgab145. J Clin Endocrinol Metab. 2021. PMID: 33693703 Free PMC article. Clinical Trial.
-
Bone Density, Geometry, Structure and Strength Estimates in Adolescent and Young Adult Women with Atypical Anorexia Nervosa versus Typical Anorexia Nervosa and Normal-Weight Healthy Controls.Nutrients. 2023 Sep 12;15(18):3946. doi: 10.3390/nu15183946. Nutrients. 2023. PMID: 37764731 Free PMC article.
-
Bone health in anorexia nervosa.Curr Opin Endocrinol Diabetes Obes. 2011 Dec;18(6):376-82. doi: 10.1097/MED.0b013e32834b4bdc. Curr Opin Endocrinol Diabetes Obes. 2011. PMID: 21897220 Free PMC article. Review.
-
Anorexia nervosa and bone.J Endocrinol. 2014 Jun;221(3):R163-76. doi: 10.1530/JOE-14-0039. J Endocrinol. 2014. PMID: 24898127 Free PMC article. Review.
Cited by
-
Loss of Bone Density in Patients with Anorexia Nervosa Food That Alone Will Not Cure.Nutrients. 2024 Oct 23;16(21):3593. doi: 10.3390/nu16213593. Nutrients. 2024. PMID: 39519426 Free PMC article. Review.
-
Gender-affirming endocrine care for youth with a nonbinary gender identity.Ther Adv Endocrinol Metab. 2023 Mar 30;14:20420188231160405. doi: 10.1177/20420188231160405. eCollection 2023. Ther Adv Endocrinol Metab. 2023. PMID: 37006780 Free PMC article. Review.
References
-
- Misra M., Aggarwal A., Miller K.K., Almazan C., Worley M., Soyka L.A., Herzog D.B., Klibanski A. Effects of anorexia nervosa on clinical, hematologic, biochemical, and bone density parameters in community-dwelling adolescent girls. Pediatrics. 2004;114:1574–1583. doi: 10.1542/peds.2004-0540. - DOI - PubMed
-
- Misra M., Prabhakaran R., Miller K.K., Goldstein M.A., Mickley D., Clauss L., Lockhart P., Cord J., Herzog D.B., Katzman D.K., et al. Weight gain and restoration of menses as predictors of bone mineral density change in adolescent girls with anorexia nervosa-1. J. Clin. Endocrinol. Metab. 2008;93:1231–1237. doi: 10.1210/jc.2007-1434. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
