

Exposure to Per- and Polyfluoroalkyl Substances and Mortality in U.S. Adults: A Population-Based Cohort Study
- PMID: 35731224
- PMCID: PMC9215707
- DOI: 10.1289/EHP10393
Exposure to Per- and Polyfluoroalkyl Substances and Mortality in U.S. Adults: A Population-Based Cohort Study
Abstract
Background: Per- and polyfluoroalkyl substances (PFAS) are widespread environmental contaminants associated with diseases such as cancer and dyslipidemia. However, few studies have investigated the association between PFAS mixture exposure and mortality in general populations.
Objectives: This study aimed to explore the association between PFAS mixture, perfluorooctanoic acid (PFOA), and perfluorooctane sulfonic acid (PFOS) and mortality in U.S. adults by a nationally representative cohort.
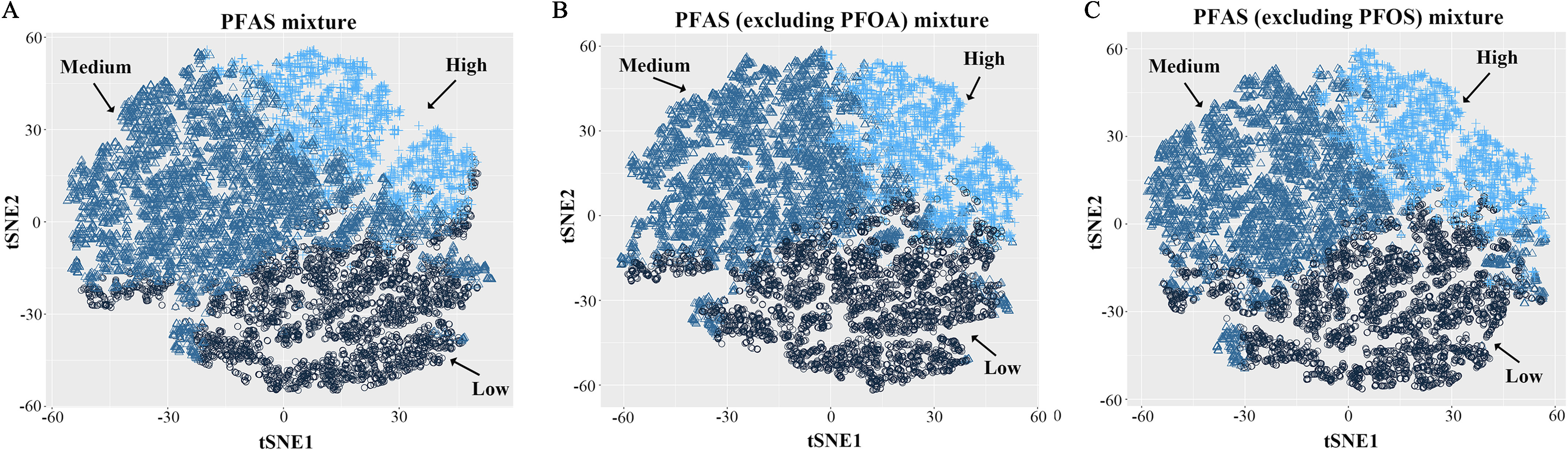
Methods: Adults of age who were enrolled in the National Health and Nutrition Examination Survey (NHANES) (1999-2014) were included in our study. Baseline serum concentrations of seven PFAS were measured and individuals were followed up to 31 December 2015. Hazard ratios (HRs) and confidence intervals (CIs) were estimated using Cox proportional hazards models. Association between PFAS mixture exposure and mortality was analyzed using the k-means method by clustering PFAS mixtures into subgroups. Association between PFOA/PFOS exposure and mortality was subsequently analyzed in both continuous and categorical models.
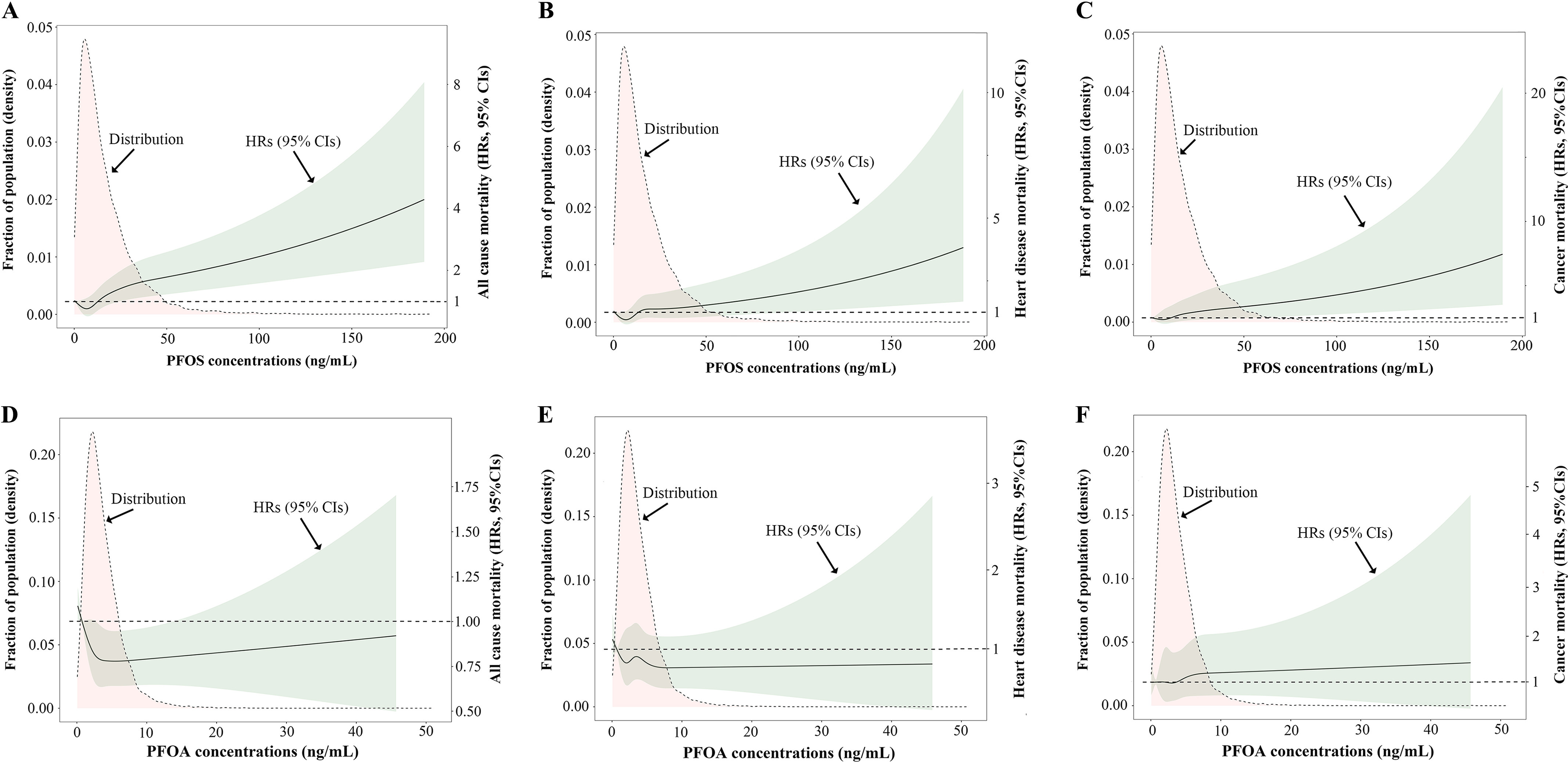
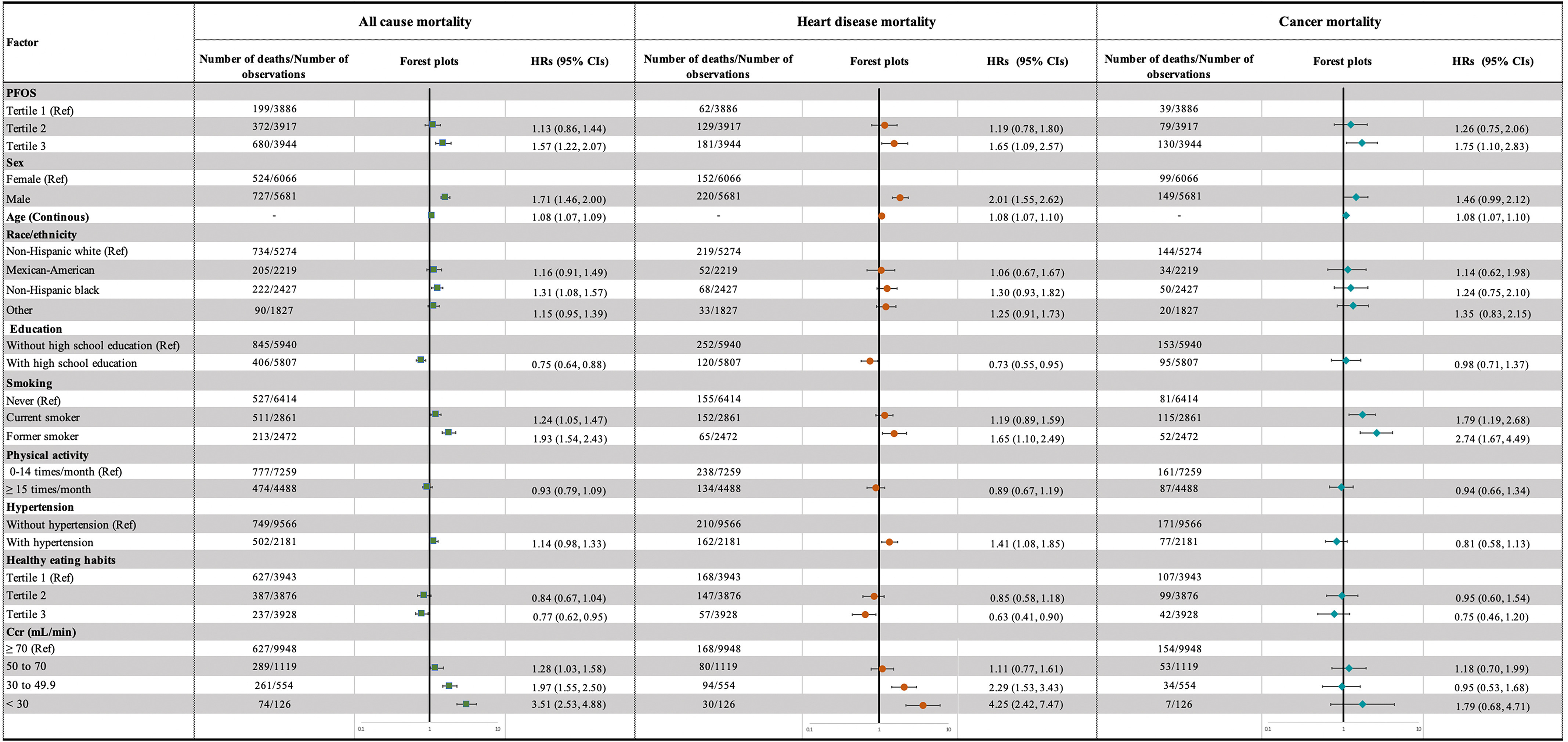
Results: During the follow-up period, 1,251 participants died. In the mixture analysis, the k-means algorithm clustered participants into low-, medium-, and high-exposure groups. Compared with the low-exposure group, participants in the high-exposure group showed significantly higher risks for all-cause mortality (; 95% CI: 1.07, 1.80), heart disease mortality (; 95% CI: 1.05, 2.51), and cancer mortality (; 95% CI: 1.08, 2.84). In single PFAS analysis, PFOS was found to be positively associated with all-cause mortality (third vs. first tertile ; 95% CI: 1.22, 2.07), heart disease mortality (third vs. first tertile ; 95% CI: 1.09, 2.57), and cancer mortality (third vs. first tertile ; 95% CI: 1.10, 2.83), whereas PFOA exposure had no significant association with mortality. Assuming the observed association is causal, the number of deaths associated with PFOS exposure ( vs. ) was (95% CI: 176,000, 588,000) annually between 1999 and 2015, and it decreased to 69,000 (95% CI: 28,000, 119,000) annually between 2015 and 2018. The association between PFOS and mortality was stronger among women and people without diabetes.
Discussion: We observed a positive association between PFAS mixture exposure and mortality among U.S. adults. Limitations of this study include the potential for unmeasured confounding, selection bias, a relatively small number of deaths, and only measuring PFAS at one point in time. Further studies with serial measures of PFAS concentrations and longer follow-ups are necessary to elucidate the association between PFAS and mortality from specific causes. https://doi.org/10.1289/EHP10393.
Figures
Similar articles
-
Exposure to per- and polyfluoroalkyl substances and age-related macular degeneration in U.S. middle-aged and older adults.Chemosphere. 2024 Sep;364:143167. doi: 10.1016/j.chemosphere.2024.143167. Epub 2024 Aug 22. Chemosphere. 2024. PMID: 39181460
-
Case-Cohort Study of the Association between PFAS and Selected Cancers among Participants in the American Cancer Society's Cancer Prevention Study II LifeLink Cohort.Environ Health Perspect. 2023 Dec;131(12):127007. doi: 10.1289/EHP13174. Epub 2023 Dec 13. Environ Health Perspect. 2023. PMID: 38088576 Free PMC article.
-
Per- and Polyfluoroalkyl Substances (PFAS) and Lipid Trajectories in Women 45-56 Years of Age: The Study of Women's Health Across the Nation.Environ Health Perspect. 2023 Aug;131(8):87004. doi: 10.1289/EHP12351. Epub 2023 Aug 8. Environ Health Perspect. 2023. PMID: 37552133 Free PMC article.
-
Associations between Per- and Polyfluoroalkyl Substances Exposures and Blood Lipid Levels among Adults-A Meta-Analysis.Environ Health Perspect. 2023 May;131(5):56001. doi: 10.1289/EHP11840. Epub 2023 May 4. Environ Health Perspect. 2023. PMID: 37141244 Free PMC article. Review.
-
Association between per- and polyfluoroalkyl substances exposure and risk of diabetes: a systematic review and meta-analysis.J Expo Sci Environ Epidemiol. 2023 Jan;33(1):40-55. doi: 10.1038/s41370-022-00464-3. Epub 2022 Aug 15. J Expo Sci Environ Epidemiol. 2023. PMID: 35970987 Review.
Cited by
-
Associations of per- and polyfluoroalkyl substances and nonalcoholic fatty liver disease in the United States adult population, 2003-2018.Environ Epidemiol. 2024 Jan 10;8(1):e284. doi: 10.1097/EE9.0000000000000284. eCollection 2024 Feb. Environ Epidemiol. 2024. PMID: 38343734 Free PMC article.
-
Trends in Serum Per- and Polyfluoroalkyl Substance (PFAS) Concentrations in Teenagers and Adults, 1999-2018 NHANES.Int J Environ Res Public Health. 2023 Oct 27;20(21):6984. doi: 10.3390/ijerph20216984. Int J Environ Res Public Health. 2023. PMID: 37947542 Free PMC article.
-
Associations of perfluoroalkyl substances with metabolic-associated fatty liver disease and non-alcoholic fatty liver disease: NHANES 2017-2018.Cancer Causes Control. 2024 Sep;35(9):1271-1282. doi: 10.1007/s10552-024-01865-5. Epub 2024 May 19. Cancer Causes Control. 2024. PMID: 38764062
-
Signaling pathways in obesity: mechanisms and therapeutic interventions.Signal Transduct Target Ther. 2022 Aug 28;7(1):298. doi: 10.1038/s41392-022-01149-x. Signal Transduct Target Ther. 2022. PMID: 36031641 Free PMC article. Review.
-
PFAS and their association with the increased risk of cardiovascular disease in postmenopausal women.Toxicol Sci. 2024 Aug 1;200(2):312-323. doi: 10.1093/toxsci/kfae065. Toxicol Sci. 2024. PMID: 38758093
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
