

Clinical efficacy of different monoclonal antibody regimens among non-hospitalised patients with mild to moderate COVID-19 at high risk for disease progression: a prospective cohort study
- PMID: 35727429
- PMCID: PMC9209841
- DOI: 10.1007/s10096-022-04464-x
Clinical efficacy of different monoclonal antibody regimens among non-hospitalised patients with mild to moderate COVID-19 at high risk for disease progression: a prospective cohort study
Abstract
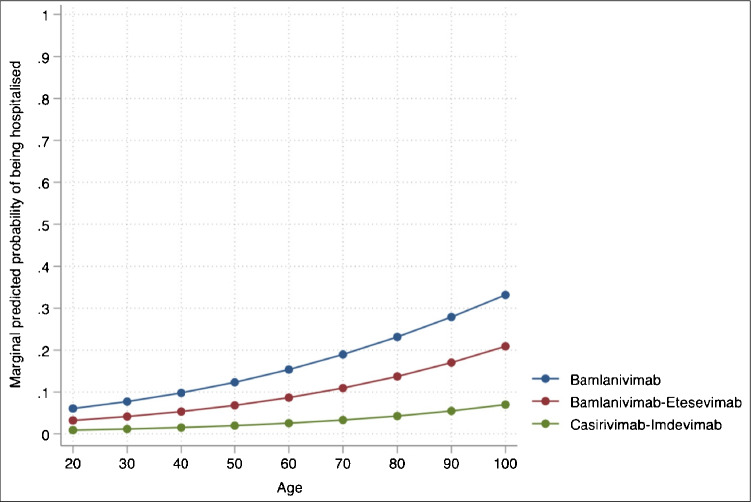
This study aimed to compare the clinical progression of COVID-19 in high-risk outpatients treated with the monoclonal antibodies (mAb) bamlanivimab, bamlanivimab-etesevimab and casirivimab-imdevimab. This is an observational, multi-centre, prospective study conducted from 18 March to 15 July 2021 in eight Italian tertiary-care hospitals including mild-to-moderate COVID-19 outpatients receiving bamlanivimab (700 mg), bamlanivimab-etesevimab (700-1400 mg) or casirivimab-imdevimab (1200-1200 mg). All patients were at high risk of COVID-19 progression according to Italian Medicines Agency definitions. In a patient subgroup, SARS-CoV-2 variant and anti-SARS-CoV-2 serology were analysed at baseline. Factors associated with 28-day all-cause hospitalisation were identified using multivariable multilevel logistic regression (MMLR) and summarised with adjusted odds ratio (aOR) and 95% confidence interval (CI). A total of 635 outpatients received mAb: 161 (25.4%) bamlanivimab, 396 (62.4%) bamlanivimab-etesevimab and 78 (12.2%) casirivimab-imdevimab. Ninety-five (15%) patients received full or partial SARS-CoV-2 vaccination. The B.1.1.7 (Alpha) variant was detected in 99% of patients. Baseline serology showed no significant differences among the three mAb regimen groups. Twenty-eight-day all-cause hospitalisation was 11.3%, with a significantly higher proportion (p 0.001) in the bamlanivimab group (18.6%), compared to the bamlanivimab-etesevimab (10.1%) and casirivimab-imdevimab (2.6%) groups. On MMLR, aORs for 28-day all-cause hospitalisation were significantly lower in patients receiving bamlanivimab-etesevimab (aOR 0.51, 95% CI 0.30-0.88 p 0.015) and casirivimab-imdevimab (aOR 0.14, 95% CI 0.03-0.61, p 0.009) compared to those receiving bamlanivimab. No patients with a history of vaccination were hospitalised. The study suggests differences in clinical outcomes among the first available mAb regimens for treating high-risk COVID-19 outpatients. Randomised trials are needed to compare efficacy of mAb combination regimens in high-risk populations and according to circulating variants.
Keywords: Bamlanivimab-etesevimab, casirivimab-imdevimab; Mild-to-moderate COVID-19 outpatients; Monoclonal antibody treatments for COVID-19; SARS-CoV-2 early treatments.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
SARS-CoV-2-neutralising monoclonal antibodies for treatment of COVID-19.Cochrane Database Syst Rev. 2021 Sep 2;9(9):CD013825. doi: 10.1002/14651858.CD013825.pub2. Cochrane Database Syst Rev. 2021. PMID: 34473343 Free PMC article. Review.
-
Curbing the Delta Surge: Clinical Outcomes After Treatment With Bamlanivimab-Etesevimab, Casirivimab-Imdevimab, or Sotrovimab for Mild to Moderate Coronavirus Disease 2019.Mayo Clin Proc. 2022 Sep;97(9):1641-1648. doi: 10.1016/j.mayocp.2022.06.015. Epub 2022 Jun 23. Mayo Clin Proc. 2022. PMID: 36058578 Free PMC article.
-
Comparison of Dual Monoclonal Antibody Therapies for COVID-19 Evolution: A Multicentric Retrospective Study.Viruses. 2024 Sep 29;16(10):1542. doi: 10.3390/v16101542. Viruses. 2024. PMID: 39459877 Free PMC article.
-
Exploratory data on the clinical efficacy of monoclonal antibodies against SARS-CoV-2 Omicron variant of concern.Elife. 2022 Nov 22;11:e79639. doi: 10.7554/eLife.79639. Elife. 2022. PMID: 36413383 Free PMC article. Clinical Trial.
-
SARS-CoV-2-neutralising monoclonal antibodies to prevent COVID-19.Cochrane Database Syst Rev. 2022 Jun 17;6(6):CD014945. doi: 10.1002/14651858.CD014945.pub2. Cochrane Database Syst Rev. 2022. PMID: 35713300 Free PMC article. Review.
Cited by
-
Functional diversification of innate and inflammatory immune responses mediated by antibody fragment crystallizable activities against SARS-CoV-2.iScience. 2024 Apr 11;27(5):109703. doi: 10.1016/j.isci.2024.109703. eCollection 2024 May 17. iScience. 2024. PMID: 38706870 Free PMC article.
-
Monoclonal Antibodies against SARS-CoV-2 Infection: Results from a Real-Life Study before the Omicron Surge.Vaccines (Basel). 2022 Nov 10;10(11):1895. doi: 10.3390/vaccines10111895. Vaccines (Basel). 2022. PMID: 36366403 Free PMC article.
-
Efficacy and safety of bamlanivimab in patients with COVID-19: A systematic review and meta-analysis.World J Virol. 2024 Mar 25;13(1):88660. doi: 10.5501/wjv.v13.i1.88660. World J Virol. 2024. PMID: 38616851 Free PMC article.
-
Host immunological responses facilitate development of SARS-CoV-2 mutations in patients receiving monoclonal antibody treatments.J Clin Invest. 2023 Mar 15;133(6):e166032. doi: 10.1172/JCI166032. J Clin Invest. 2023. PMID: 36727404 Free PMC article.
References
-
- Agenzia A (2011) AIFA - Agenzia Italiana del Farmaco DETERMINA 17 marzo 2021. 1–4
-
- Agenzia A (2011) AIFA - Agenzia Italiana del Farmaco DETERMINA 22 marzo 2021. 1–4
-
- Agenzia A (2011) AIFA - Agenzia Italiana del Farmaco DETERMINA 9 marzo 2021. 1–4.
-
- Gottlieb RL, Nirula A, Chen P, Boscia J, Heller B, Morris J, et al. Effect of bamlanivimab as monotherapy or in combination with etesevimab on viral load in patients with mild to moderate COVID-19: a randomized clinical trial. JAMA - J Am Med Assoc. 2021;325(7):632–644. doi: 10.1001/jama.2021.0202. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Miscellaneous
