

The Prognostic Signature and Therapeutic Value of Phagocytic Regulatory Factors in Prostate Adenocarcinoma (PRAD)
- PMID: 35706452
- PMCID: PMC9190300
- DOI: 10.3389/fgene.2022.877278
The Prognostic Signature and Therapeutic Value of Phagocytic Regulatory Factors in Prostate Adenocarcinoma (PRAD)
Abstract
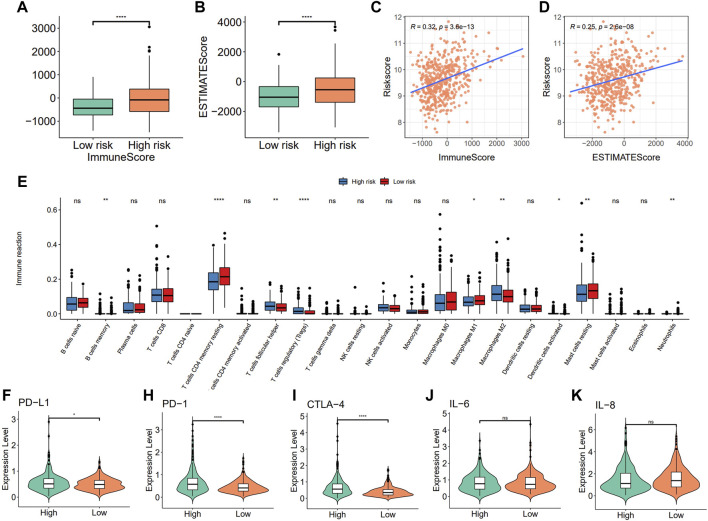
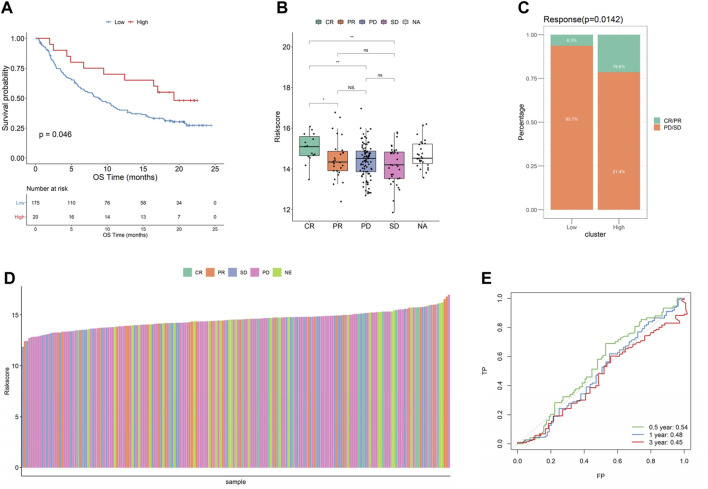
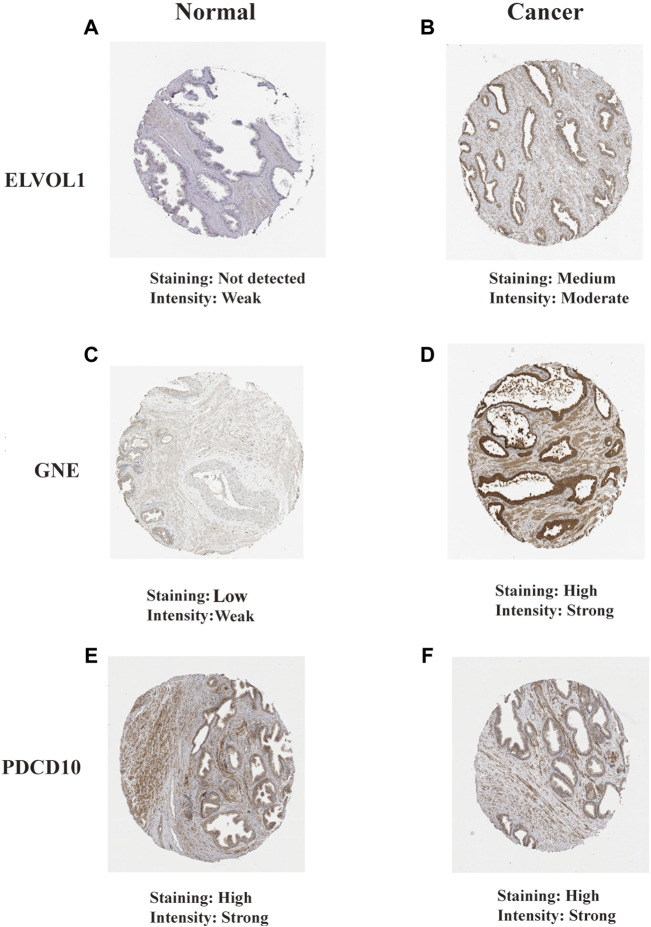
There is growing evidence that phagocytosis regulatory factors (PRFs) play important roles in tumor progression, and therefore, identifying and characterizing these factors is crucial for understanding the mechanisms of cellular phagocytosis in tumorigenesis. Our research aimed to comprehensively characterize PRFs in prostate adenocarcinoma (PRAD) and to screen and determine important PRFs in PRAD which may help to inform tumor prognostic and therapeutic signatures based on these key PRFs. Here, we first systematically described the expression of PRFs in PRAD and evaluated their expression patterns and their prognostic value. We then analyzed prognostic phagocytic factors by Cox and Lasso analysis and constructed a phagocytic factor-mediated risk score. We then divided the samples into two groups with significant differences in overall survival (OS) based on the risk score. Then, we performed correlation analysis between the risk score and clinical features, immune infiltration levels, immune characteristics, immune checkpoint expression, IC50 of several classical sensitive drugs, and immunotherapy efficacy. Finally, the Human Protein Atlas (HPA) database was used to determine the protein expression of 18 PRF characteristic genes. The aforementioned results confirmed that multilayer alterations of PRFs were associated with the prognosis of patients with PRAD and the degree of macrophage infiltration. These findings may provide us with potential new therapies for PRAD.
Keywords: PRAD; immune infiltration; phagocytic factor; prostate cancer; survival analysis.
Copyright © 2022 Xin, Sun, Jin, Li, Liu, Zhou and Ye.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
The novel transcriptomic signature of angiogenesis predicts clinical outcome, tumor microenvironment and treatment response for prostate adenocarcinoma.Mol Med. 2022 Jul 14;28(1):78. doi: 10.1186/s10020-022-00504-6. Mol Med. 2022. PMID: 35836112 Free PMC article.
-
A N7-Methylguanine-Related Gene Signature Applicable for the Prognosis and Microenvironment of Prostate Cancer.J Oncol. 2022 May 13;2022:8604216. doi: 10.1155/2022/8604216. eCollection 2022. J Oncol. 2022. PMID: 35602299 Free PMC article.
-
Identification of Prognostic Biomarkers Associated with Cancer Stem Cell Features in Prostate Adenocarcinoma.Med Sci Monit. 2020 Jul 31;26:e924543. doi: 10.12659/MSM.924543. Med Sci Monit. 2020. PMID: 32735556 Free PMC article.
-
Long non-coding RNA profile study identifies an immune-related lncRNA prognostic signature for prostate adenocarcinoma.Int Immunopharmacol. 2021 Dec;101(Pt A):108267. doi: 10.1016/j.intimp.2021.108267. Epub 2021 Nov 2. Int Immunopharmacol. 2021. PMID: 34740081
-
Development of a novel five-gene immune-related risk model for the prognosis evaluation of prostate adenocarcinoma patients.Am J Cancer Res. 2022 May 15;12(5):2337-2349. eCollection 2022. Am J Cancer Res. 2022. PMID: 35693084 Free PMC article.
Cited by
-
LncRNA CTBP1-AS inhibits TP63-mediated activation of S100A14 during prostate cancer progression.Cancer Sci. 2024 May;115(5):1492-1504. doi: 10.1111/cas.16138. Epub 2024 Mar 13. Cancer Sci. 2024. PMID: 38476086 Free PMC article.
-
Analysis and identification of the necroptosis landscape on therapy and prognosis in bladder cancer.Front Genet. 2022 Sep 29;13:919829. doi: 10.3389/fgene.2022.919829. eCollection 2022. Front Genet. 2022. PMID: 36246597 Free PMC article.
-
Mechanism of TCF21 Downregulation Leading to Immunosuppression of Tumor-Associated Macrophages in Non-Small Cell Lung Cancer.Pharmaceutics. 2023 Sep 7;15(9):2295. doi: 10.3390/pharmaceutics15092295. Pharmaceutics. 2023. PMID: 37765264 Free PMC article.
-
DARS expression in BCR/ABL1-negative myeloproliferative neoplasms and its association with the immune microenvironment.Sci Rep. 2024 Jul 19;14(1):16711. doi: 10.1038/s41598-024-67067-w. Sci Rep. 2024. PMID: 39030308 Free PMC article.
References
LinkOut - more resources
Full Text Sources