

Early Steps of Resistance to Targeted Therapies in Non-Small-Cell Lung Cancer
- PMID: 35681591
- PMCID: PMC9179469
- DOI: 10.3390/cancers14112613
Early Steps of Resistance to Targeted Therapies in Non-Small-Cell Lung Cancer
Abstract
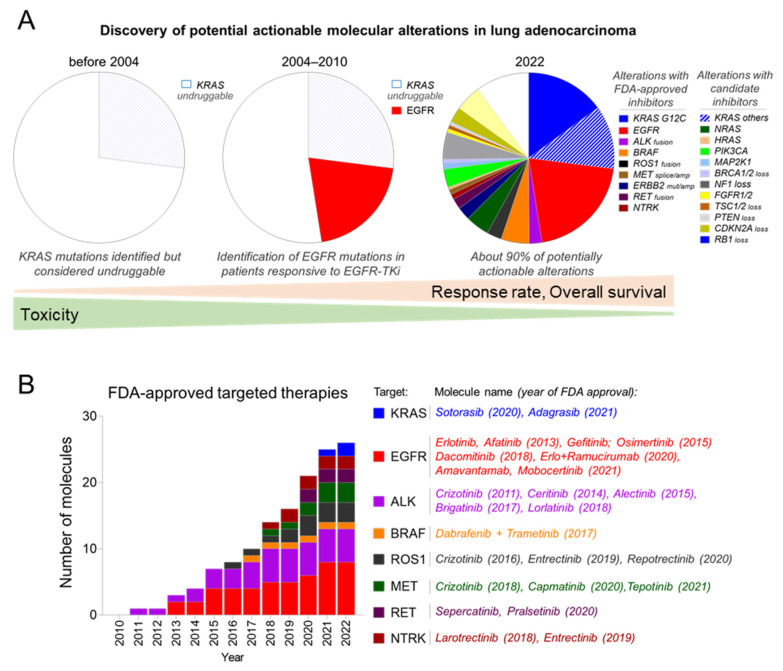
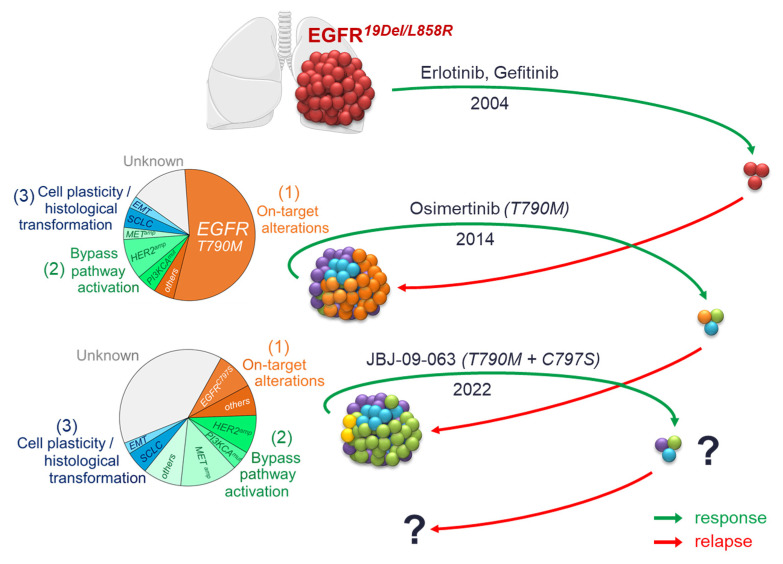
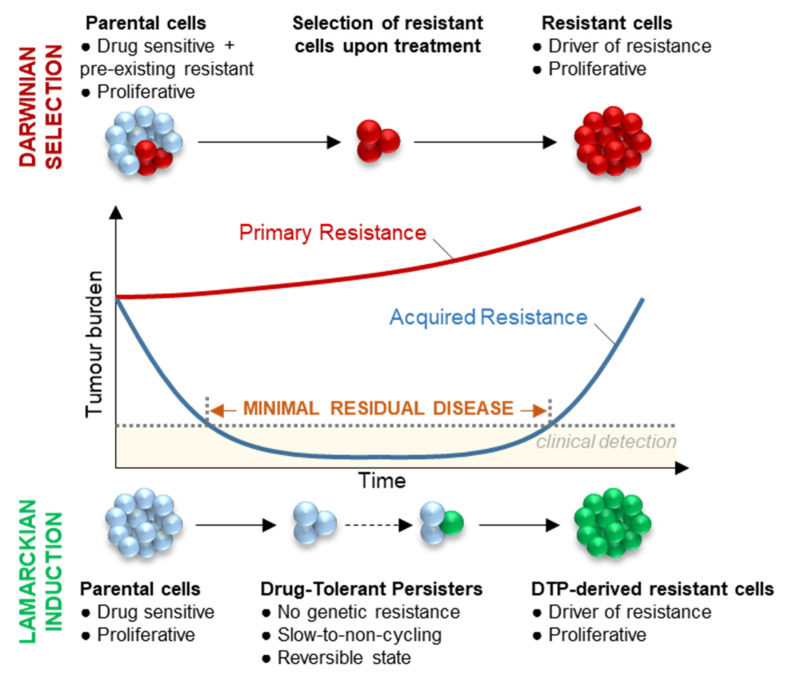
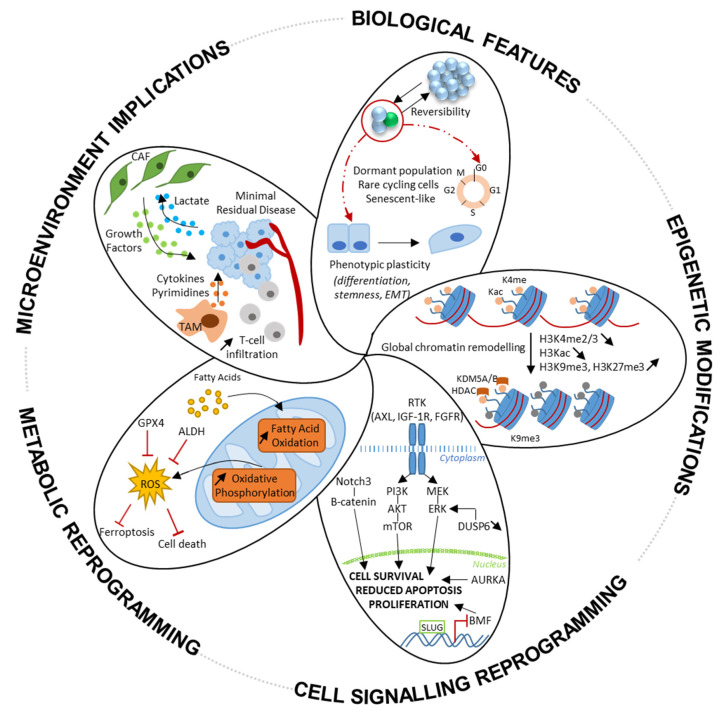
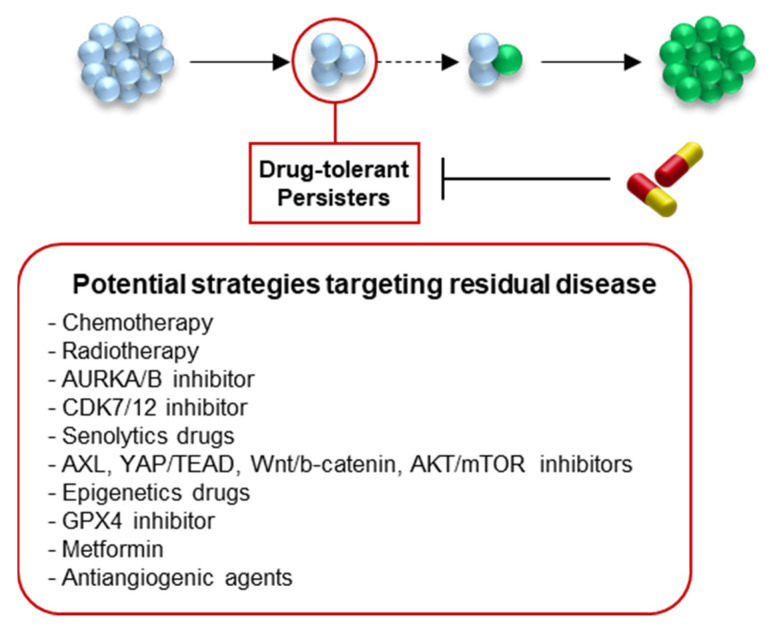
Lung cancer is the leading cause of cancer-related deaths among men and women worldwide. Epidermal growth factor receptor-tyrosine kinase inhibitors (EGFR-TKIs) are effective therapies for advanced non-small-cell lung cancer (NSCLC) patients harbouring EGFR-activating mutations, but are not curative due to the inevitable emergence of resistances. Recent in vitro studies suggest that resistance to EGFR-TKI may arise from a small population of drug-tolerant persister cells (DTP) through non-genetic reprogramming, by entering a reversible slow-to-non-proliferative state, before developing genetically derived resistances. Deciphering the molecular mechanisms governing the dynamics of the drug-tolerant state is therefore a priority to provide sustainable therapeutic solutions for patients. An increasing number of molecular mechanisms underlying DTP survival are being described, such as chromatin and epigenetic remodelling, the reactivation of anti-apoptotic/survival pathways, metabolic reprogramming, and interactions with their micro-environment. Here, we review and discuss the existing proposed mechanisms involved in the DTP state. We describe their biological features, molecular mechanisms of tolerance, and the therapeutic strategies that are tested to target the DTP.
Keywords: EGFR-TKI; drug-tolerant persisters; lung cancer; targeted therapies.
Conflict of interest statement
Julien Mazieres reports personal fees from Astra Zeneca, BMS, MSD, Novartis, Amgen, and grants from Roche, Astra Zeneca, Pierre Fabre, BMS. The other authors declare no conflict of interest.
Figures
Similar articles
-
Mechanisms of Acquired Resistance and Tolerance to EGFR Targeted Therapy in Non-Small Cell Lung Cancer.Cancers (Basel). 2023 Jan 13;15(2):504. doi: 10.3390/cancers15020504. Cancers (Basel). 2023. PMID: 36672453 Free PMC article. Review.
-
Mechanism of Drug Tolerant Persister Cancer Cells: The Landscape and Clinical Implication for Therapy.J Thorac Oncol. 2021 Nov;16(11):1798-1809. doi: 10.1016/j.jtho.2021.07.017. Epub 2021 Aug 3. J Thorac Oncol. 2021. PMID: 34352380 Review.
-
EMT: A mechanism for escape from EGFR-targeted therapy in lung cancer.Biochim Biophys Acta Rev Cancer. 2019 Jan;1871(1):29-39. doi: 10.1016/j.bbcan.2018.10.003. Epub 2018 Nov 10. Biochim Biophys Acta Rev Cancer. 2019. PMID: 30419315 Review.
-
Combined blockade of GPX4 and activated EGFR/HER3 bypass pathways inhibits the development of ALK-inhibitor-induced tolerant persister cells in ALK-fusion-positive lung cancer.Mol Oncol. 2024 Oct 6. doi: 10.1002/1878-0261.13746. Online ahead of print. Mol Oncol. 2024. PMID: 39369284
-
Targeting FGFR overcomes EMT-mediated resistance in EGFR mutant non-small cell lung cancer.Oncogene. 2019 Sep;38(37):6399-6413. doi: 10.1038/s41388-019-0887-2. Epub 2019 Jul 19. Oncogene. 2019. PMID: 31324888 Free PMC article.
Cited by
-
Targeting HER3 to overcome EGFR TKI resistance in NSCLC.Front Immunol. 2024 Jan 4;14:1332057. doi: 10.3389/fimmu.2023.1332057. eCollection 2023. Front Immunol. 2024. PMID: 38239350 Free PMC article. Review.
-
SOS1 and KSR1 modulate MEK inhibitor responsiveness to target resistant cell populations based on PI3K and KRAS mutation status.Proc Natl Acad Sci U S A. 2023 Nov 21;120(47):e2313137120. doi: 10.1073/pnas.2313137120. Epub 2023 Nov 16. Proc Natl Acad Sci U S A. 2023. PMID: 37972068 Free PMC article.
-
Investigating the role of prognostic mitophagy-related genes in non-small cell cancer pathogenesis via multiomics and network-based approach.3 Biotech. 2024 Nov;14(11):273. doi: 10.1007/s13205-024-04127-y. Epub 2024 Oct 21. 3 Biotech. 2024. PMID: 39444988
-
The Third Joint Meeting on Lung Cancer of the FHU OncoAge (University Côte d'Azur, Nice, France) and the University of Texas MD Anderson Cancer Center (Houston, TX, USA). Understanding New Therapeutic Options and Promising Predictive Biomarkers for Lung Cancer Patients.Cancers (Basel). 2022 Sep 4;14(17):4327. doi: 10.3390/cancers14174327. Cancers (Basel). 2022. PMID: 36077862 Free PMC article.
-
Farnesyltransferase inhibition overcomes oncogene-addicted non-small cell lung cancer adaptive resistance to targeted therapies.Nat Commun. 2024 Jun 27;15(1):5345. doi: 10.1038/s41467-024-49360-4. Nat Commun. 2024. PMID: 38937474 Free PMC article.
References
-
- Allemani C., Matsuda T., Di Carlo V., Harewood R., Matz M., Nikšić M., Bonaventure A., Valkov M., Johnson C.J., Estève J., et al. Global surveillance of trends in cancer survival 2000–14 (CONCORD-3): Analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018;391:1023–1075. doi: 10.1016/S0140-6736(17)33326-3. - DOI - PMC - PubMed
-
- Barlesi F., Mazieres J., Merlio J.-P., Debieuvre D., Mosser J., Lena H., Ouafik L.H., Besse B., Rouquette I., Westeel V., et al. Routine molecular profiling of patients with advanced non-small-cell lung cancer: Results of a 1-year nationwide programme of the French Cooperative Thoracic Intergroup (IFCT) Lancet. 2016;387:1415–1426. doi: 10.1016/S0140-6736(16)00004-0. - DOI - PubMed
-
- Jordan E.J., Kim H.R., Arcila M.E., Barron D., Chakravarty D., Gao J., Chang M.T., Ni A., Kundra R., Jonsson P., et al. Prospective Comprehensive Molecular Characterization of Lung Adenocarcinomas for Efficient Patient Matching to Approved and Emerging Therapies. Cancer Discov. 2017;7:596–609. doi: 10.1158/2159-8290.CD-16-1337. - DOI - PMC - PubMed
-
- Rosell R., Carcereny E., Gervais R., Vergnenegre A., Massuti B., Felip E., Palmero R., Garcia-Gomez R., Pallares C., Sanchez J.M., et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13:239–246. doi: 10.1016/S1470-2045(11)70393-X. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
