

Genetic and Pharmacological Disruption of Interleukin-1α Leads to Augmented Murine Aortic Aneurysm
- PMID: 35680012
- PMCID: PMC11029039
- DOI: 10.1016/j.avsg.2022.05.024
Genetic and Pharmacological Disruption of Interleukin-1α Leads to Augmented Murine Aortic Aneurysm
Abstract
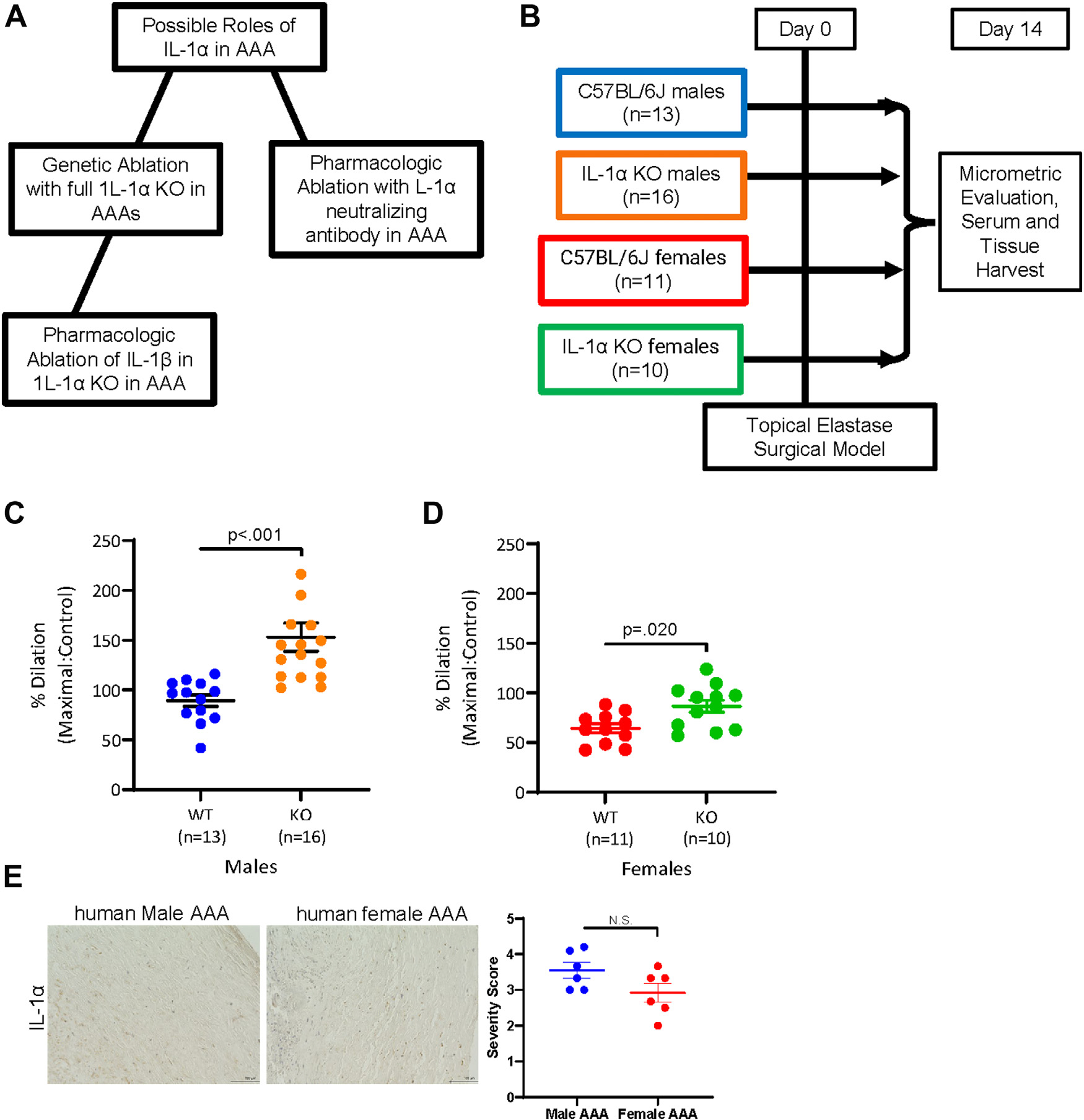
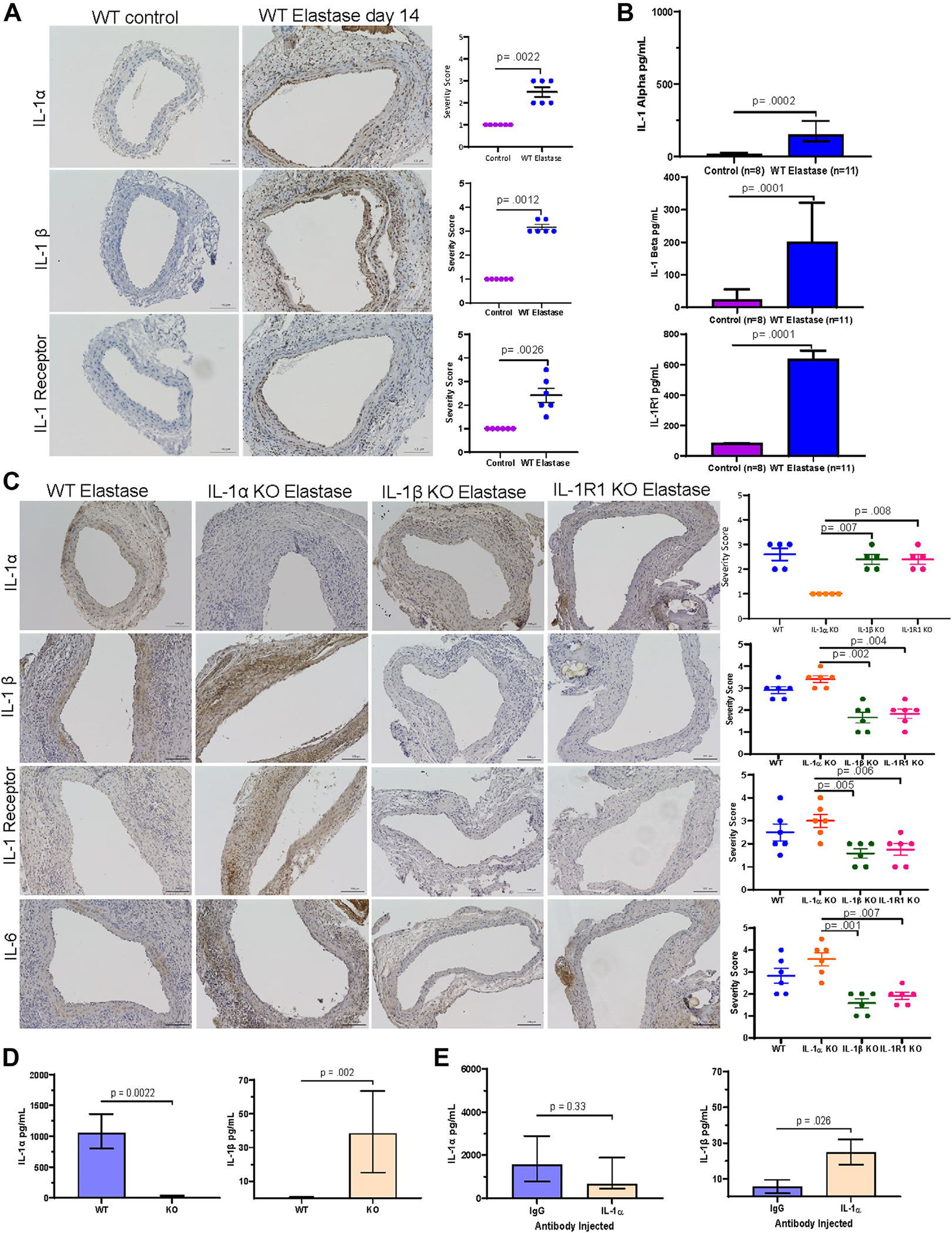
Background: Interleukin-1 (IL-1) signaling has an established role as a cytokine signaling pathway important for progression of abdominal aortic aneurysms (AAAs). While the IL-1β ligand and IL-1R1 have been previously investigated, the role of the IL-1α ligand in AAAs remains unknown. In this study, we sought to examine the role of IL-1α in AAAs using genetic and pharmacologic approaches.
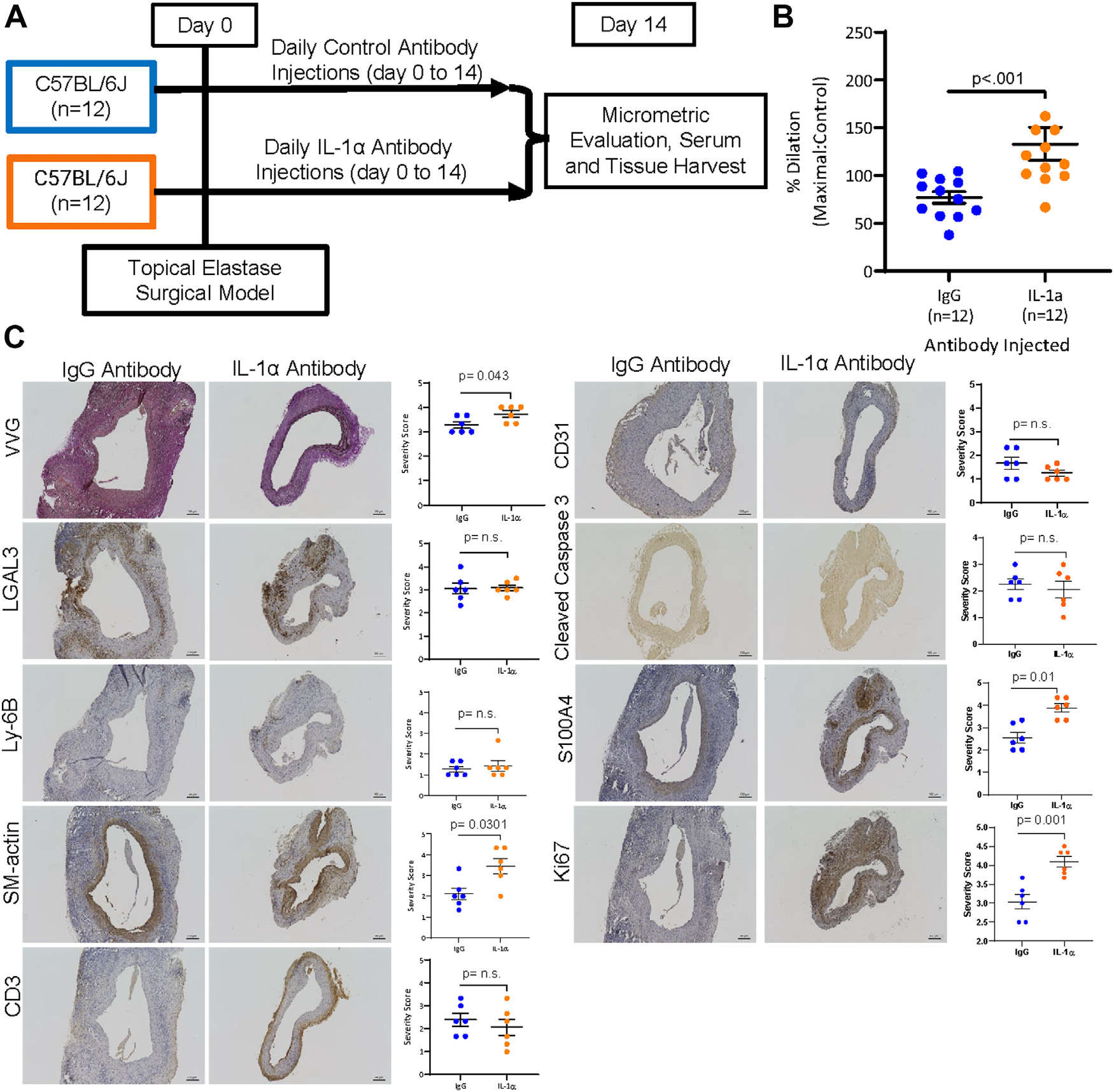
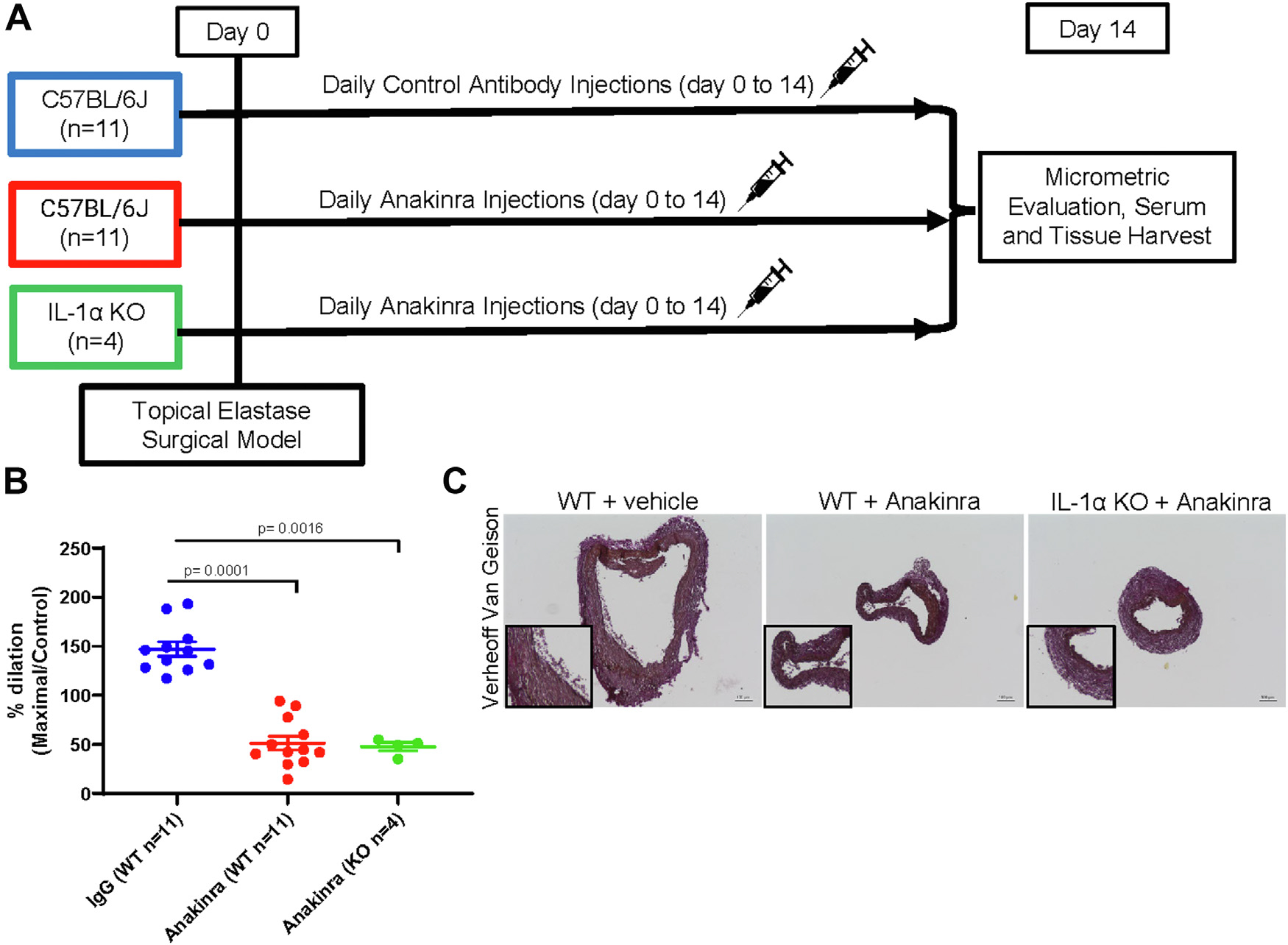
Methods: Eight-week-old wild-type (WT) or IL-1α knock-out (KO) male and female mice (n = 10-16/group) underwent experimental AAA and were harvested 14 days following surgery to assess AAA size and characteristics. In separate studies, 8-week-old WT mice were treated with an inhibitor to IL-1α during AAA formation and harvested 14 days following surgery. Finally, WT and IL-1α KO mice were administered Anakinra, an IL-R1 inhibitor, during AAA formation to determine the effect of inhibiting IL-1R1 when IL-1α is knocked out.
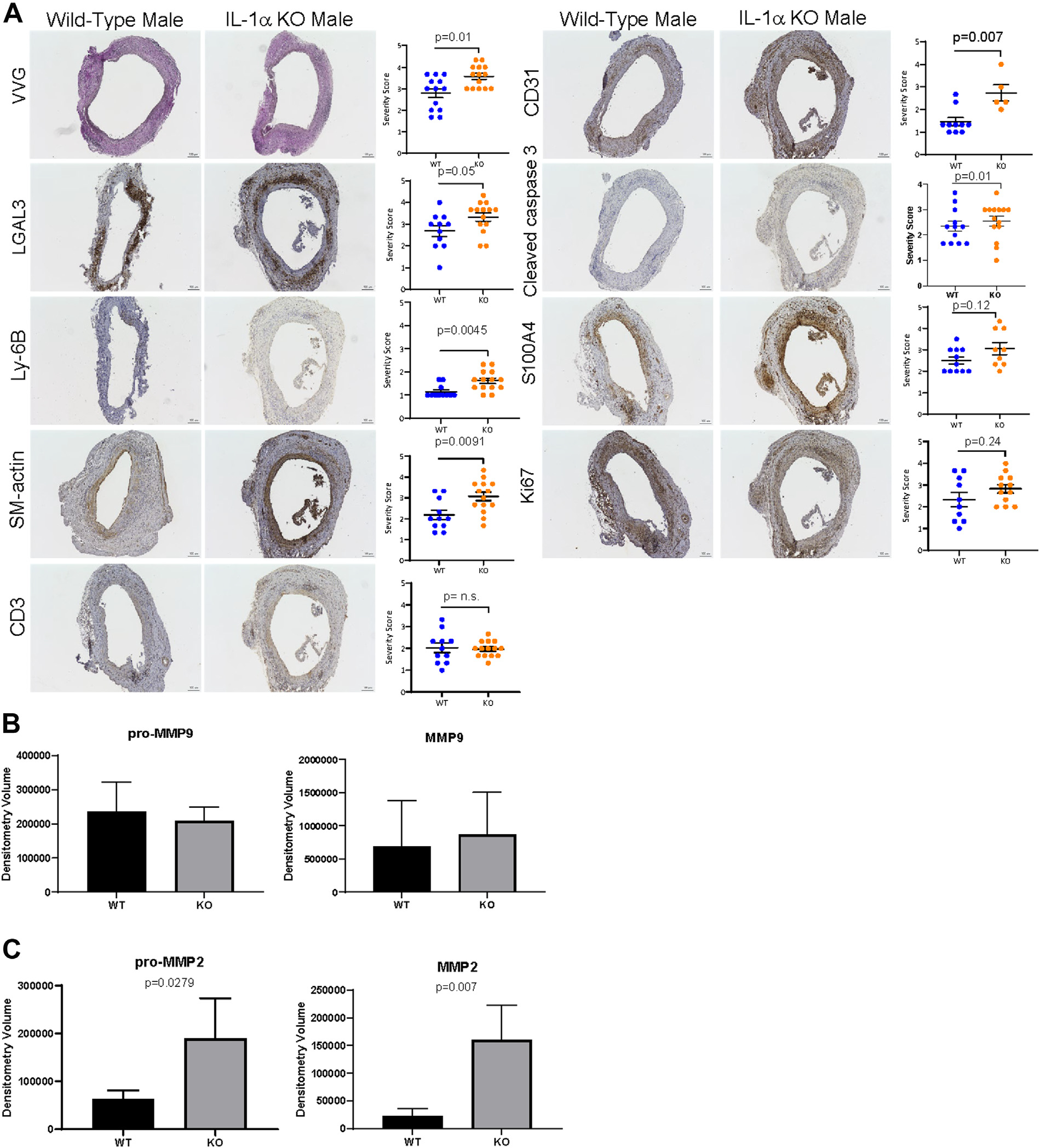
Results: Male and female IL-1α KO mice had larger AAAs compared to WT AAAs (male: 153% vs. 89.2%, P = 0.0001; female: 86.6% vs. 63.5%, P = 0.02). IL-1α KO mice had greater elastin breakage (P = 0.01), increased levels of macrophage staining (P = 0.0045), and greater pro-metallo proteinase 2 (P = 0.02). Pharmacologic inhibition of WT male mice with an IL-1α neutralizing antibody resulted in larger AAAs (133.1% vs. 77.0%, P < 0.001). Finally, treatment of IL-1α KO male mice with Anakinra decreased AAA formation compared with vehicle control AAAs (Anakinra + IL-1α KO: 47.7% vs. WT: 147.1%; P = 0.0001).
Conclusions: IL-1α disruption using either genetic or pharmacologic approaches worsens AAAs.
Copyright © 2022 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Genetic and pharmacologic disruption of interleukin-1β signaling inhibits experimental aortic aneurysm formation.Arterioscler Thromb Vasc Biol. 2013 Feb;33(2):294-304. doi: 10.1161/ATVBAHA.112.300432. Epub 2013 Jan 3. Arterioscler Thromb Vasc Biol. 2013. PMID: 23288154 Free PMC article.
-
Role of Interleukin-1 Signaling in a Mouse Model of Kawasaki Disease-Associated Abdominal Aortic Aneurysm.Arterioscler Thromb Vasc Biol. 2016 May;36(5):886-97. doi: 10.1161/ATVBAHA.115.307072. Epub 2016 Mar 3. Arterioscler Thromb Vasc Biol. 2016. PMID: 26941015 Free PMC article.
-
Inhibition of interleukin-1β decreases aneurysm formation and progression in a novel model of thoracic aortic aneurysms.Circulation. 2014 Sep 9;130(11 Suppl 1):S51-9. doi: 10.1161/CIRCULATIONAHA.113.006800. Circulation. 2014. PMID: 25200056 Free PMC article.
-
Pharmacologic blockade and genetic deletion of androgen receptor attenuates aortic aneurysm formation.J Vasc Surg. 2016 Jun;63(6):1602-1612.e2. doi: 10.1016/j.jvs.2015.11.038. Epub 2016 Jan 24. J Vasc Surg. 2016. PMID: 26817611 Free PMC article.
-
Hypoxia-inducible factor 1 in clinical and experimental aortic aneurysm disease.J Vasc Surg. 2018 Nov;68(5):1538-1550.e2. doi: 10.1016/j.jvs.2017.09.030. Epub 2017 Dec 11. J Vasc Surg. 2018. PMID: 29242064 Free PMC article.
Cited by
-
IL-1 in Abdominal Aortic Aneurysms.J Cell Immunol. 2023;5(2):22-31. doi: 10.33696/immunology.5.163. J Cell Immunol. 2023. PMID: 37476160 Free PMC article.
-
A highly selective mPGES-1 inhibitor to block abdominal aortic aneurysm progression in the angiotensin mouse model.Sci Rep. 2024 Mar 23;14(1):6959. doi: 10.1038/s41598-024-57437-9. Sci Rep. 2024. PMID: 38521811 Free PMC article.
References
-
- Lindholt JS, Vammen S, Juul S, et al. The validity of ultrasonographic scanning as screening method for abdominal aortic aneurysm. Eur J Vasc Endovasc Surg 1999;17:472–5. - PubMed
-
- Norman PE, Semmens JB, Lawrence-Brown MMD. Long-term relative survival following surgery for abdominal aortic aneurysm: a review. Cardiovasc Surg 2001;9:219–24. - PubMed
-
- Scott RA, Wilson NM, Ashton HA, et al. Influence of screening on the incidence of ruptured abdominal aortic aneurysm: 5-year results of a randomized controlled study. Br J Surg 1995;82:1066–70. - PubMed
-
- Scott RAP, Bridgewater SG, Ashton HA. Randomized clinical trial of screening for abdominal aortic aneurysm in women. Br J Surg 2002;89:283–5. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Research Materials
