

Comparative incidence of early and late bloodstream and respiratory tract co-infection in patients admitted to ICU with COVID-19 pneumonia versus Influenza A or B pneumonia versus no viral pneumonia: wales multicentre ICU cohort study
- PMID: 35655224
- PMCID: PMC9160852
- DOI: 10.1186/s13054-022-04026-9
Comparative incidence of early and late bloodstream and respiratory tract co-infection in patients admitted to ICU with COVID-19 pneumonia versus Influenza A or B pneumonia versus no viral pneumonia: wales multicentre ICU cohort study
Abstract
Objective: The aim is to characterise early and late respiratory and bloodstream co-infection in patients admitted to intensive care units (ICUs) with SARS-CoV-2-related acute hypoxemic respiratory failure (AHRF) needing respiratory support in seven ICUs within Wales, during the first wave of the COVID-19 pandemic. We compare the rate of positivity of different secondary pathogens and their antimicrobial sensitivity in three different patient groups: patients admitted to ICU with COVID-19 pneumonia, Influenza A or B pneumonia, and patients without viral pneumonia.
Design: Multicentre, retrospective, observational cohort study with rapid microbiology data from Public Health Wales, sharing of clinical and demographic data from seven participating ICUs.
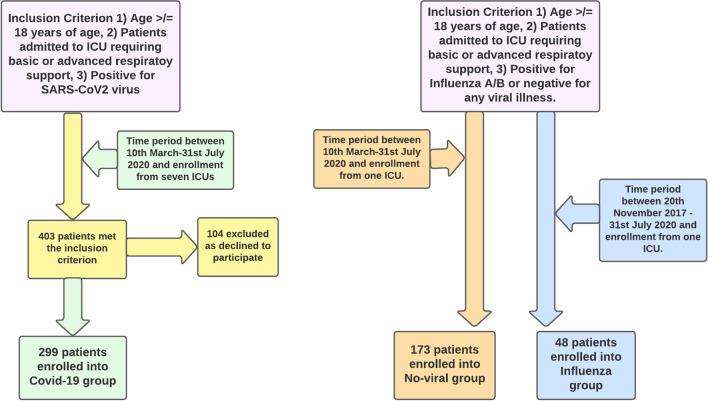
Setting: Seven Welsh ICUs participated between 10 March and 31 July 2020. Clinical and demographic data for COVID-19 disease were shared by each participating centres, and microbiology data were extracted from a data repository within Public Health Wales. Comparative data were taken from a cohort of patients without viral pneumonia admitted to ICU during the same period as the COVID-19 cohort (referred to as no viral pneumonia or 'no viral' group), and to a retrospective non-matched cohort of consecutive patients with Influenza A or B admitted to ICUs from 20 November 2017. The comparative data for Influenza pneumonia and no viral pneumonia were taken from one of the seven participating ICUs.
Participants: A total of 299 consecutive patients admitted to ICUs with COVID-19 pneumonia were compared with 173 and 48 patients admitted with no viral pneumonia or Influenza A or B pneumonia, respectively.
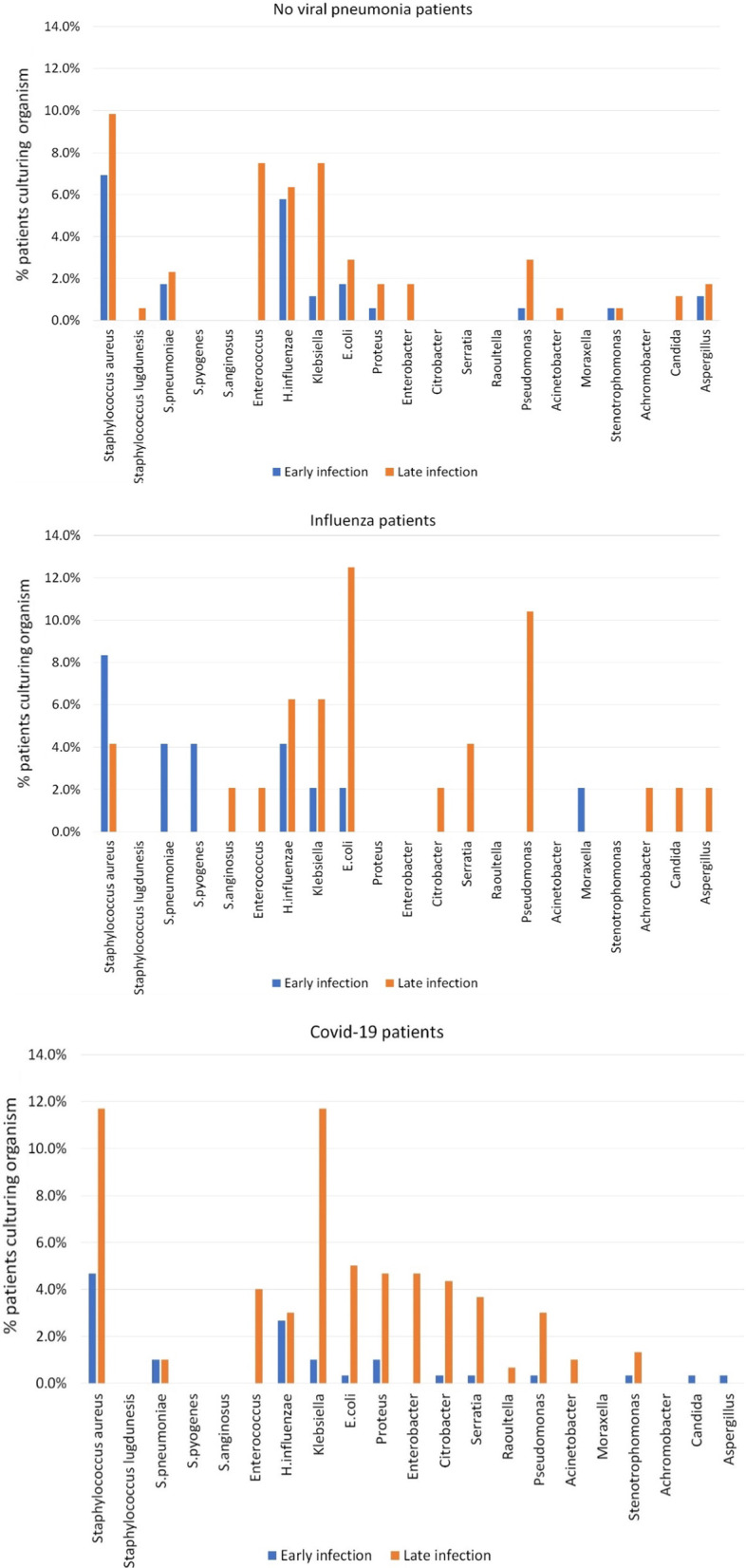
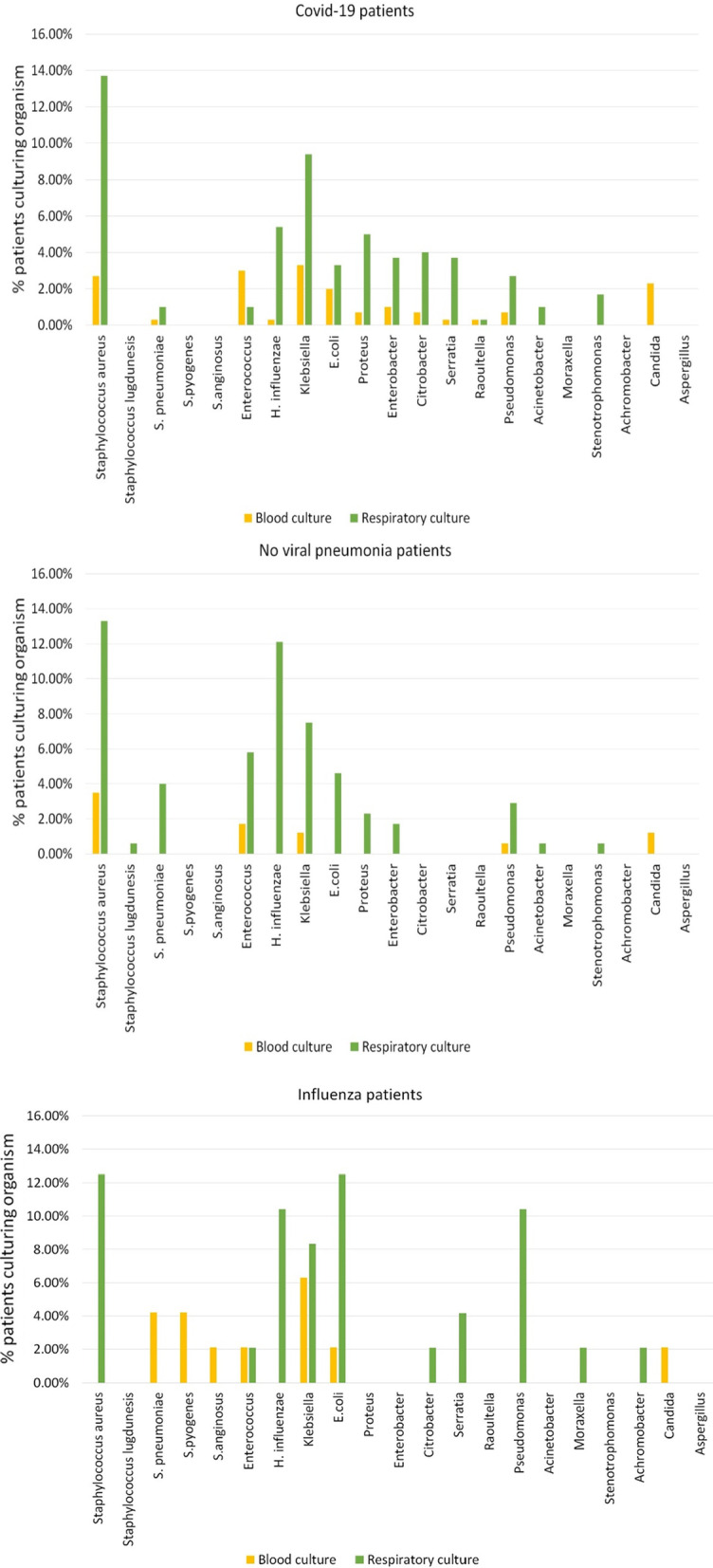
Main outcome measures: Primary outcome was to calculate comparative incidence of early and late co-infection in patients admitted to ICU with COVID-19, Influenza A or B pneumonia and no viral pneumonia. Secondary outcome was to calculate the individual group of early and late co-infection rate on a per-patient and per-sample basis, with their antimicrobial susceptibility and thirdly to ascertain any statistical correlation between clinical and demographic variables with rate of acquiring co-infection following ICU admission.
Results: A total of 299 adults (median age 57, M/F 2:1) were included in the COVID-19 ICU cohort. The incidence of respiratory and bloodstream co-infection was 40.5% and 15.1%, respectively. Staphylococcus aureus was the predominant bacterial pathogen within the first 48 h. Gram-negative organisms from Enterobacterales group were predominantly seen after 48 h in COVID-19 cohort. Comparative no viral pneumonia cohort had lower rates of respiratory tract infection and bloodstream infection. The influenza cohort had similar rates respiratory tract infection and bloodstream infection. Mortality in all three groups was similar, and no clinical or demographic variables were found to increase the rate of co-infection and ICU mortality.
Conclusions: Higher incidence of bacterial co-infection was found in COVID-19 cohort as compared to the no viral pneumonia cohort admitted to ICUs for respiratory support.
Keywords: Antibiotic sensitivity; Aspergillus; COVID-19; Co-infection; Early; Influenza A and B; Late; SARS-CoV-2.
© 2022. The Author(s).
Conflict of interest statement
All authors declare that they have no competing interests.
Figures
Similar articles
-
Bloodstream infections in the era of the COVID-19 pandemic: Changing epidemiology of antimicrobial resistance in the intensive care unit.J Intensive Med. 2024 Mar 27;4(3):269-280. doi: 10.1016/j.jointm.2023.12.004. eCollection 2024 Jul. J Intensive Med. 2024. PMID: 39035613 Free PMC article. Review.
-
Bacterial and fungal coinfection among hospitalized patients with COVID-19: a retrospective cohort study in a UK secondary-care setting.Clin Microbiol Infect. 2020 Oct;26(10):1395-1399. doi: 10.1016/j.cmi.2020.06.025. Epub 2020 Jun 27. Clin Microbiol Infect. 2020. PMID: 32603803 Free PMC article.
-
Secondary infections in critically ill patients with viral pneumonia due to COVID-19 and influenza: a historical cohort study.Can J Anaesth. 2023 Mar;70(3):374-383. doi: 10.1007/s12630-022-02376-0. Epub 2023 Mar 14. Can J Anaesth. 2023. PMID: 36918454 Free PMC article.
-
Co-infection in critically ill patients with COVID-19: an observational cohort study from England.J Med Microbiol. 2021 Apr;70(4):001350. doi: 10.1099/jmm.0.001350. J Med Microbiol. 2021. PMID: 33861190 Free PMC article.
-
Assessing respiratory viral exclusion and affinity interactions through co-infection incidence in a pediatric population during the 2022 resurgence of influenza and RSV.Front Cell Infect Microbiol. 2023 Jun 14;13:1208235. doi: 10.3389/fcimb.2023.1208235. eCollection 2023. Front Cell Infect Microbiol. 2023. PMID: 37389220 Free PMC article. Review.
Cited by
-
Coinfection and superinfection in ICU critically ill patients with severe COVID-19 pneumonia and influenza pneumonia: are the pictures different?Front Public Health. 2023 Aug 29;11:1195048. doi: 10.3389/fpubh.2023.1195048. eCollection 2023. Front Public Health. 2023. PMID: 37711242 Free PMC article.
-
Bloodstream Infections in Intensive Care Unit during Four Consecutive SARS-CoV-2 Pandemic Waves.Antibiotics (Basel). 2023 Sep 14;12(9):1448. doi: 10.3390/antibiotics12091448. Antibiotics (Basel). 2023. PMID: 37760744 Free PMC article.
-
Impact of COVID-19 on healthcare-associated infections: Antimicrobial consumption does not follow antimicrobial resistance.Clinics (Sao Paulo). 2023 Jun 13;78:100231. doi: 10.1016/j.clinsp.2023.100231. eCollection 2023. Clinics (Sao Paulo). 2023. PMID: 37348255 Free PMC article.
-
Bloodstream infections in the era of the COVID-19 pandemic: Changing epidemiology of antimicrobial resistance in the intensive care unit.J Intensive Med. 2024 Mar 27;4(3):269-280. doi: 10.1016/j.jointm.2023.12.004. eCollection 2024 Jul. J Intensive Med. 2024. PMID: 39035613 Free PMC article. Review.
-
Secondary pulmonary infection and co-infection in elderly COVID-19 patients during the pandemics in a tertiary general hospital in Beijing, China.Front Microbiol. 2023 Oct 12;14:1280026. doi: 10.3389/fmicb.2023.1280026. eCollection 2023. Front Microbiol. 2023. PMID: 37901822 Free PMC article.
References
-
- https://public.tableau.com/views/RapidCOVID-19virology-Public/Headlinesu.... Public health Wales health-protection profile.
-
- Randolph AG, Vaughn F, Sullivan R, Rubinson L, Thompson BT, Yoon G, Smoot E, Rice TW, Loftis LL, Helfaer M, Doctor A, Paden M, Flori H, Babbitt C, Graciano AL, Gedeit R, Sanders RC, Giuliano JS, Zimmerman J. Pediatric Acute Lung Injury and Sepsis Investigator's Network and the National Heart, Lung, and Blood Institute ARDS Clinical Trials Network. Critically ill children during the 2009–2010 influenza pandemic in the United States. Pediatrics. 2011;128(6):e1450–e1458. doi: 10.1542/peds.2011-0774. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
