

Coronary Artery Calcification Score and the Progression of Chronic Kidney Disease
- PMID: 35654602
- PMCID: PMC9342644
- DOI: 10.1681/ASN.2022010080
Coronary Artery Calcification Score and the Progression of Chronic Kidney Disease
Abstract
Background: An elevated coronary artery calcification score (CACS) is associated with increased cardiovascular disease risk in patients with CKD. However, the relationship between CACS and CKD progression has not been elucidated.
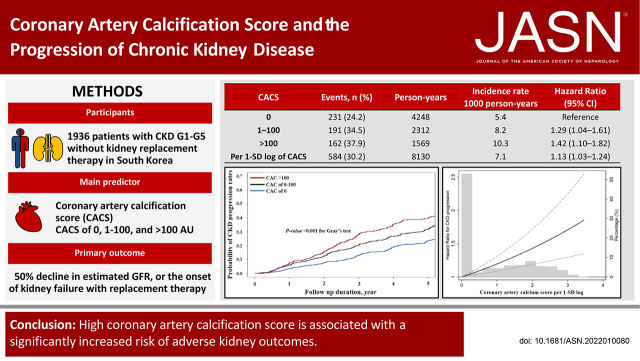
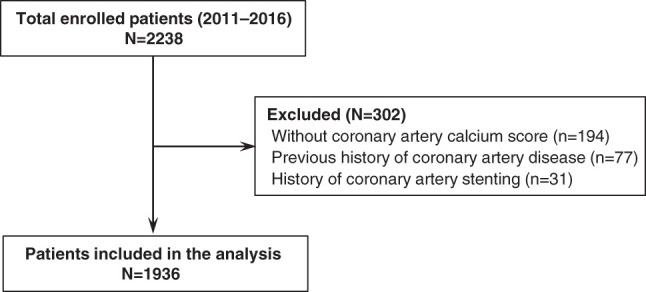
Methods: We studied 1936 participants with CKD (stages G1-G5 without kidney replacement therapy) enrolled in the KoreaN Cohort Study for Outcome in Patients With CKD. The main predictor was Agatston CACS categories at baseline (0 AU, 1-100 AU, and >100 AU). The primary outcome was CKD progression, defined as a ≥50% decline in eGFR or the onset of kidney failure with replacement therapy.
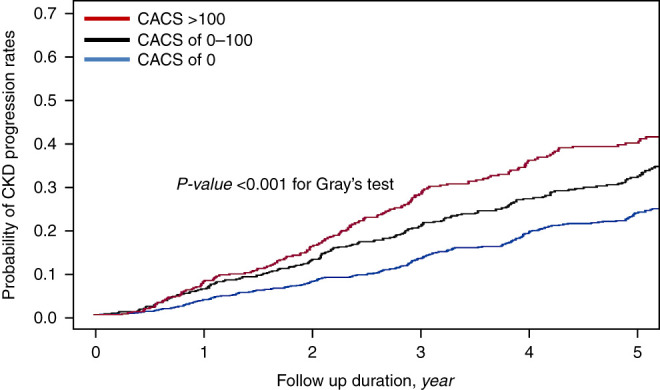
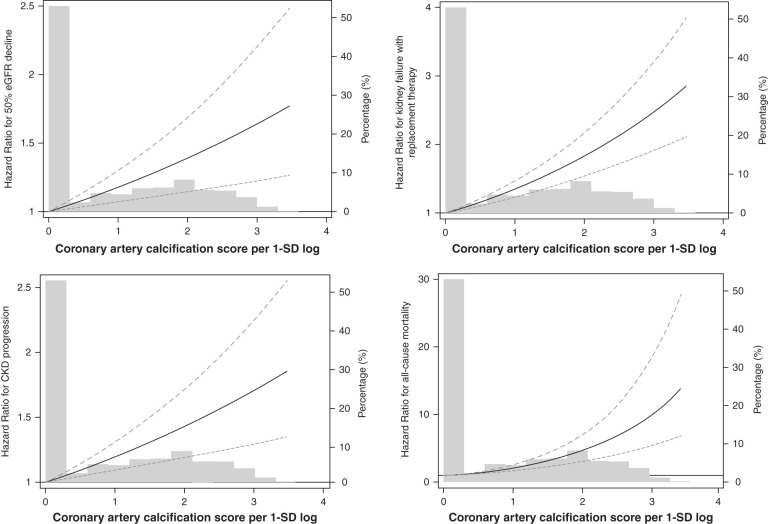
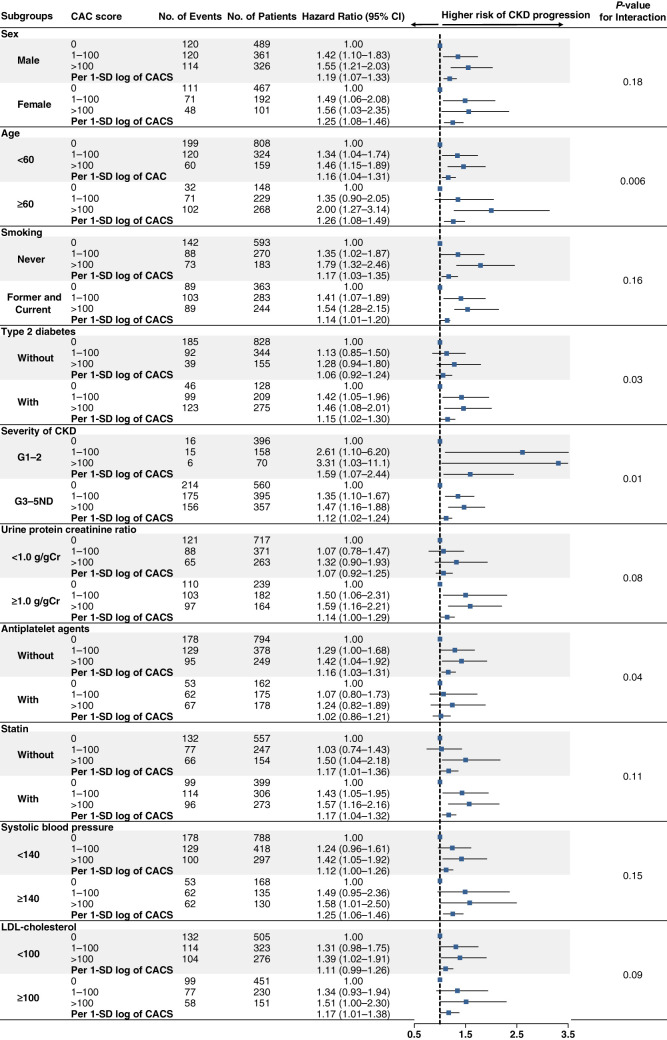
Results: During 8130 person-years of follow-up, the primary outcome occurred in 584 (30.2%) patients. In the adjusted cause-specific hazard model, CACS of 1-100 AU (hazard ratio [HR], 1.29; 95% confidence interval [CI], 1.04 to 1.61) and CACS >100 AU (HR, 1.42; 95% CI, 1.10 to 1.82) were associated with a significantly higher risk of the primary outcome. The HR associated with per 1-SD log of CACS was 1.13 (95% CI, 1.03 to 1.24). When nonfatal cardiovascular events were treated as a time-varying covariate, CACS of 1-100 AU (HR, 1.31; 95% CI, 1.07 to 1.60) and CACS >100 AU (HR, 1.46; 95% CI, 1.16 to 1.85) were also associated with a higher risk of CKD progression. The association was stronger in older patients, in those with type 2 diabetes, and in those not using antiplatelet drugs. Furthermore, patients with higher CACS had a significantly larger eGFR decline rate.
Conclusion: Our findings suggest that a high CACS is associated with significantly increased risk of adverse kidney outcomes and CKD progression.
Keywords: chronic renal disease; clinical nephrology; coronary artery disease; coronary calcification; vascular calcification.
Copyright © 2022 by the American Society of Nephrology.
Figures
Similar articles
-
Coronary artery calcification score and common iliac artery calcification score in non-dialysis CKD patients.Nephrology (Carlton). 2018 Sep;23(9):837-845. doi: 10.1111/nep.13113. Epub 2018 Feb 20. Nephrology (Carlton). 2018. PMID: 28703899 Free PMC article.
-
Association of coronary artery calcium with adverse cardiovascular outcomes and death in patients with chronic kidney disease: results from the KNOW-CKD.Nephrol Dial Transplant. 2023 Feb 28;38(3):712-721. doi: 10.1093/ndt/gfac194. Nephrol Dial Transplant. 2023. PMID: 35689669
-
Association between progression of coronary artery calcification and development of kidney failure with replacement therapy: Findings from KNOW-CKD study.Atherosclerosis. 2024 Aug;395:117563. doi: 10.1016/j.atherosclerosis.2024.117563. Epub 2024 Apr 23. Atherosclerosis. 2024. PMID: 38692977
-
Additive prognostic value of coronary artery calcium score and renal function in patients with acute chest pain without known coronary artery disease: up to 5-year follow-up.Int J Cardiovasc Imaging. 2015 Dec;31(8):1619-26. doi: 10.1007/s10554-015-0732-9. Epub 2015 Aug 5. Int J Cardiovasc Imaging. 2015. PMID: 26243534
-
Early referral strategies for management of people with markers of renal disease: a systematic review of the evidence of clinical effectiveness, cost-effectiveness and economic analysis.Health Technol Assess. 2010 Apr;14(21):1-184. doi: 10.3310/hta14210. Health Technol Assess. 2010. PMID: 20441712 Review.
Cited by
-
Association between the neutrophil-to-lymphocyte ratio and in-hospital mortality in patients with chronic kidney disease and coronary artery disease in the intensive care unit.Eur J Med Res. 2024 Apr 30;29(1):260. doi: 10.1186/s40001-024-01850-3. Eur J Med Res. 2024. PMID: 38689359 Free PMC article.
-
Progression of Vascular Calcification and Clinical Outcomes in Patients Receiving Maintenance Dialysis.JAMA Netw Open. 2023 May 1;6(5):e2310909. doi: 10.1001/jamanetworkopen.2023.10909. JAMA Netw Open. 2023. PMID: 37126347 Free PMC article.
-
Is coronary artery calcium an independent risk factor for white matter hyperintensity?BMC Neurol. 2023 Aug 30;23(1):313. doi: 10.1186/s12883-023-03364-7. BMC Neurol. 2023. PMID: 37648961 Free PMC article.
-
Pathophysiology and Clinical Impacts of Chronic Kidney Disease on Coronary Artery Calcification.J Cardiovasc Dev Dis. 2023 May 10;10(5):207. doi: 10.3390/jcdd10050207. J Cardiovasc Dev Dis. 2023. PMID: 37233174 Free PMC article. Review.
-
Effects of Finerenone on Cardiovascular and Chronic Kidney Diseases: A New Weapon against Cardiorenal Morbidity and Mortality-A Comprehensive Review.J Cardiovasc Dev Dis. 2023 May 28;10(6):236. doi: 10.3390/jcdd10060236. J Cardiovasc Dev Dis. 2023. PMID: 37367401 Free PMC article. Review.
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY: Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med 351: 1296–1305, 2004 - PubMed
-
- Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, et al. ; Chronic Kidney Disease Prognosis Consortium : Association of estimated glomerular filtration rate and albuminuria with all-cause and cardiovascular mortality in general population cohorts: A collaborative meta-analysis. Lancet 375: 2073–2081, 2010 - PMC - PubMed
-
- Tonelli M, Wiebe N, Culleton B, House A, Rabbat C, Fok M, et al. : Chronic kidney disease and mortality risk: A systematic review. J Am Soc Nephrol 17: 2034–2047, 2006 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
