

Would the Addition of Immunotherapy Impact the Prognosis of Patients With Malignant Pericardial Effusion?
- PMID: 35600364
- PMCID: PMC9120828
- DOI: 10.3389/fonc.2022.871132
Would the Addition of Immunotherapy Impact the Prognosis of Patients With Malignant Pericardial Effusion?
Abstract
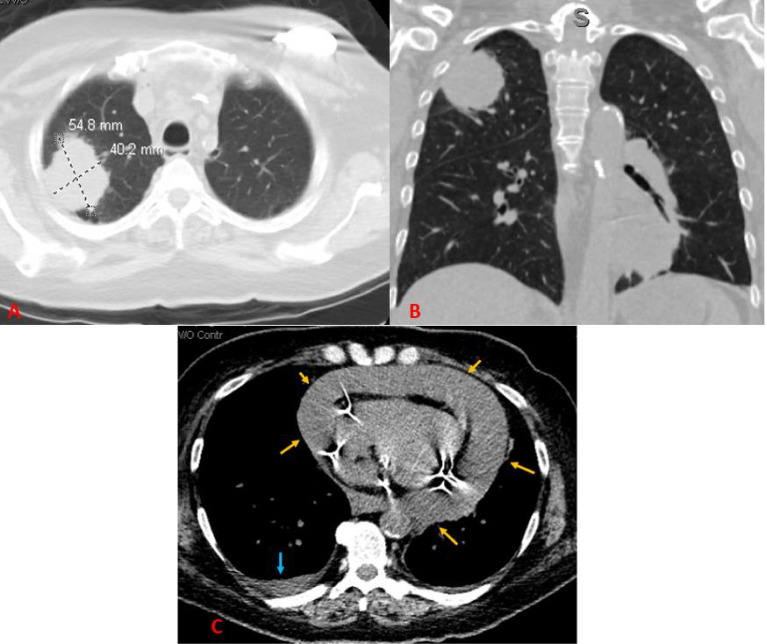
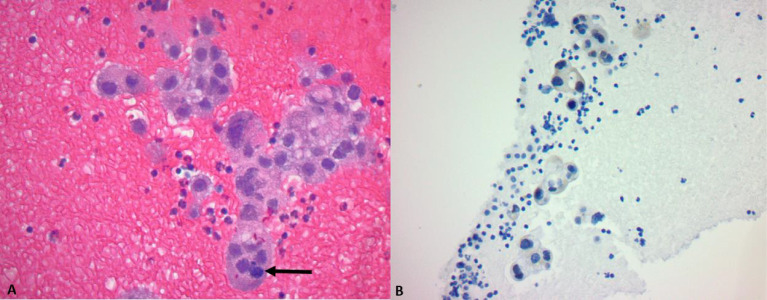
Pericardial effusion is a common finding in advanced-stage lung cancer. The presence of malignant cells or drainage of exudate effusion in the pericardial space may cause symptoms of dyspnea, pleuritic chest pain, and syncope. In addition to the difficulty physicians face in the detection and diagnosis of malignant pericardial effusion, treatment may be challenging considering the cancer prognosis and cardiovascular stability of the patient. Despite the availability of several treatment modalities for malignant pericardial effusion, including chemotherapy and surgery, patients with lung cancer historically present with poor prognoses. In addition to lung adenocarcinoma with malignant pericardial effusion, this case was complicated by COVID-19 and malignancy-associated obstructive pneumonia. We present a case of a 64-year-old woman with advanced non-small cell lung carcinoma (NSCLC) with malignant pericardial effusion who, despite testing positive for COVID-19 and having obstructive pneumonia, had favorable outcomes following systemic therapy with combined chemo-immunotherapy.
Keywords: adenocarcinoma; combined chemoimmunotherapy; immunotherapy; malignant pericardial effusion; pneumonia.
Copyright © 2022 Chiruvella, Ullah, Elhelf, Patel and Karim.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Malignant Pericardial Effusion Presenting as a Sequela of Lung Adenocarcinoma.Cureus. 2024 Mar 30;16(3):e57287. doi: 10.7759/cureus.57287. eCollection 2024 Mar. Cureus. 2024. PMID: 38690490 Free PMC article.
-
Primary Lung Adenocarcinoma Presenting as Cardiac Tamponade in a 40-Year-Old Non-Smoker.Cureus. 2022 Jan 26;14(1):e21631. doi: 10.7759/cureus.21631. eCollection 2022 Jan. Cureus. 2022. PMID: 35228977 Free PMC article.
-
Prognostic factors for malignant pericardial effusion treated by pericardial drainage in solid-malignancy patients.Med Oncol. 2007;24(4):425-30. doi: 10.1007/s12032-007-0033-9. Med Oncol. 2007. PMID: 17917093
-
Case report: malignant pericardial effusion as the initial manifestation of malignancy.Am J Med Sci. 1993 Feb;305(2):106-10. doi: 10.1097/00000441-199302000-00009. Am J Med Sci. 1993. PMID: 8427291 Review.
-
Treatment of malignant pericardial effusion.JAMA. 1994 Jul 6;272(1):59-64. JAMA. 1994. PMID: 8007081 Review.
Cited by
-
Malignant Pericardial Effusion Presenting as a Sequela of Lung Adenocarcinoma.Cureus. 2024 Mar 30;16(3):e57287. doi: 10.7759/cureus.57287. eCollection 2024 Mar. Cureus. 2024. PMID: 38690490 Free PMC article.
References
LinkOut - more resources
Full Text Sources