

Fcγ-Receptor-Based Enzyme-Linked Immunosorbent Assays for Sensitive, Specific, and Persistent Detection of Anti-SARS-CoV-2 Nucleocapsid Protein IgG Antibodies in Human Sera
- PMID: 35574677
- PMCID: PMC9199419
- DOI: 10.1128/jcm.00075-22
Fcγ-Receptor-Based Enzyme-Linked Immunosorbent Assays for Sensitive, Specific, and Persistent Detection of Anti-SARS-CoV-2 Nucleocapsid Protein IgG Antibodies in Human Sera
Abstract
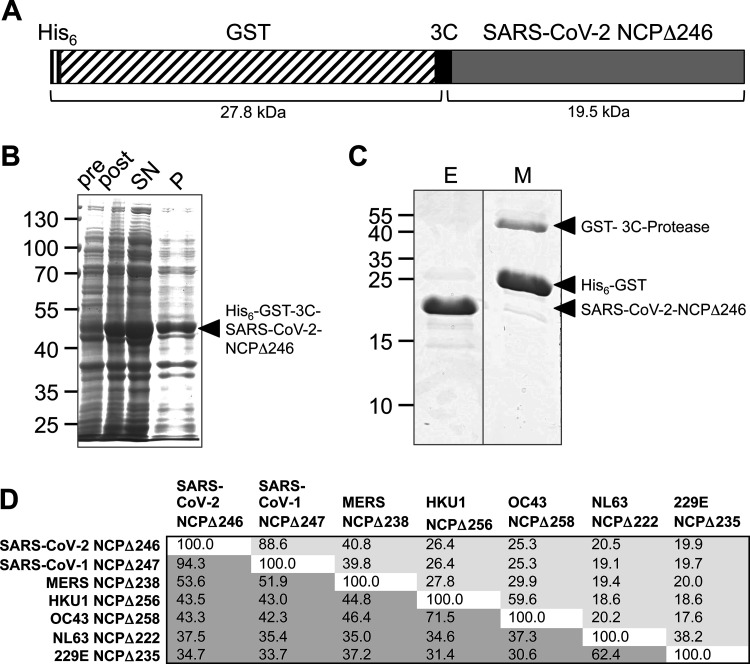
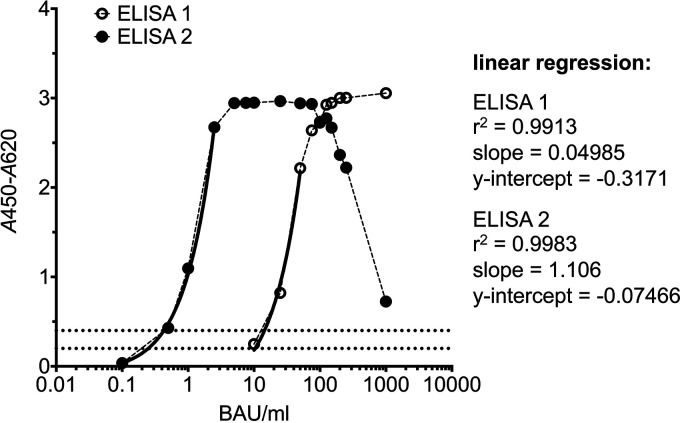
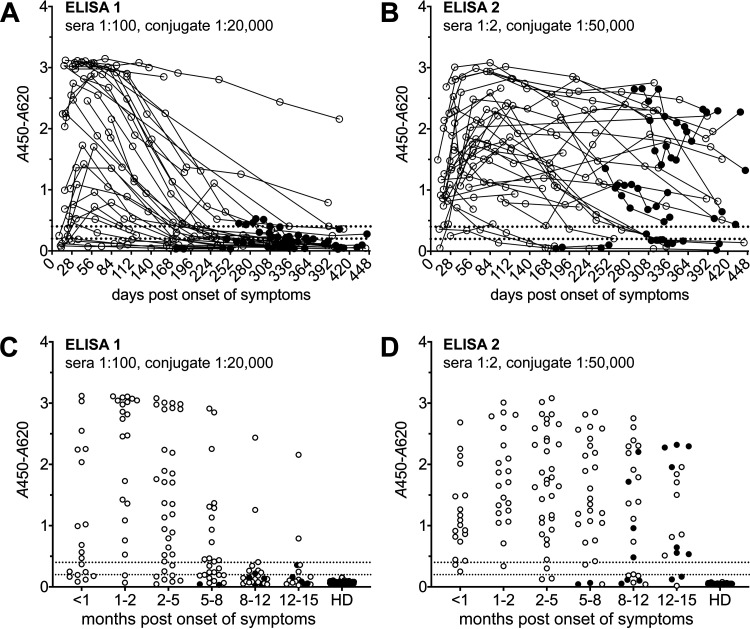
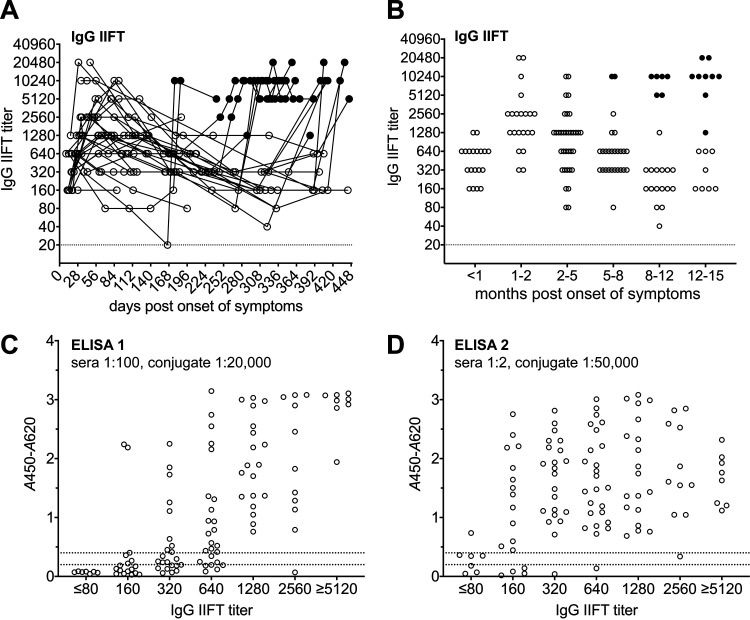
Sensitive and specific serological tests are mandatory for epidemiological studies evaluating severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) prevalence as well as coronavirus disease 2019 (COVID-19) morbidity and mortality rates. The accuracy of results is challenged by antibody waning after convalescence and by cross-reactivity induced by previous infections with other pathogens. By employing a patented platform technology based on capturing antigen-antibody complexes with a solid-phase-bound Fcγ receptor (FcγR) and truncated nucleocapsid protein as the antigen, two SARS-CoV-2 IgG enzyme-linked immunosorbent assays (ELISAs), featuring different serum and antigen dilutions, were developed. Validation was performed using a serum panel comprising 213 longitudinal samples from 35 COVID-19 patients and a negative-control panel consisting of 790 pre-COVID-19 samples from different regions of the world. While both assays show similar diagnostic sensitivities in the early convalescent phase, ELISA 2 (featuring a higher serum concentration) enables SARS-CoV-2 IgG antibody detection for a significantly longer time postinfection (≥15 months). Correspondingly, analytical sensitivity referenced to indirect immunofluorescence testing (IIFT) is significantly higher for ELISA 2 in samples with a titer of ≤1:640; for high-titer samples, a prozone effect is observed for ELISA 2. The specificities of both ELISAs were excellent not only for pre-COVID-19 serum samples from Europe, Asia, and South America but also for several challenging African sample panels. The SARS-CoV-2 IgG FcγR ELISAs, methodically combining antigen-antibody binding in solution and isotype-specific detection of immune complexes, are valuable tools for seroprevalence studies requiring the (long-term) detection of anti-SARS-CoV-2 IgG antibodies in populations with a challenging immunological background and/or in which spike-protein-based vaccine programs have been rolled out.
Keywords: immunoassay; immunoglobulins; infectious disease; laboratory methods and tools; viral diseases.
Conflict of interest statement
The authors declare a conflict of interest. Research Funding: C. Deschermeier, German Federal Ministry of Education and Research (grant no. 01KI20210) and European Regional Development Fund (ERDF) (grant no. BWF/H/52228/2012/13.10.10-1/3.4,6) to institution; P. Emmerich, German Federal Ministry of Education and Research (grant no. 01KI20210) to institution; L. Oestereich: Leibniz Association (grant no. J59/20218) to institution. Patents: C. Deschermeier, EP3207375; P. Emmerich, EP2492689, EP3207375. Other financial or non-financial interests: C. Deschermeier and B. Rushton are cofounders and shareholders of Panadea Diagnostics GmbH. Role of Sponsor: The funding organizations played no role in the design of study, choice of enrolled patients, review and interpretation of data, preparation of manuscript, or final approval of manuscript. No other Potential Conflicts of Interest have been declared.
Figures
Similar articles
-
Limited specificity of commercially available SARS-CoV-2 IgG ELISAs in serum samples of African origin.Trop Med Int Health. 2021 Jun;26(6):621-631. doi: 10.1111/tmi.13569. Epub 2021 Apr 5. Trop Med Int Health. 2021. PMID: 33666297 Free PMC article.
-
Evaluation of a SARS-CoV-2 Capture IgM Antibody Assay in Convalescent Sera.Microbiol Spectr. 2021 Oct 31;9(2):e0045821. doi: 10.1128/Spectrum.00458-21. Epub 2021 Sep 8. Microbiol Spectr. 2021. PMID: 34494855 Free PMC article.
-
Evaluation of a multiplexed coronavirus antigen array for detection of SARS-CoV-2 specific IgG in COVID-19 convalescent plasma.J Immunol Methods. 2021 Oct;497:113104. doi: 10.1016/j.jim.2021.113104. Epub 2021 Jul 22. J Immunol Methods. 2021. PMID: 34303688 Free PMC article.
-
Performance of Elecsys Anti-SARS CoV-2 (Roche) and VIDAS Anti-SARS CoV-2 (Biomérieux) for SARS-CoV-2 Nucleocapsid and Spike Protein Antibody Detection.EJIFCC. 2022 Aug 8;33(2):159-165. eCollection 2022 Aug. EJIFCC. 2022. PMID: 36313907 Free PMC article. Review.
-
SARS-CoV-2 nucleocapsid: Biological functions and implication for disease diagnosis and vaccine design.Rev Med Virol. 2023 May;33(3):e2431. doi: 10.1002/rmv.2431. Epub 2023 Feb 15. Rev Med Virol. 2023. PMID: 36790816 Review.
Cited by
-
Clinical usefulness of testing for severe acute respiratory syndrome coronavirus 2 antibodies.Eur J Intern Med. 2023 Jan;107:7-16. doi: 10.1016/j.ejim.2022.11.009. Epub 2022 Nov 10. Eur J Intern Med. 2023. PMID: 36379820 Free PMC article. Review.
-
High seroprevalence of SARS-CoV-2 in Burkina-Faso, Ghana and Madagascar in 2021: a population-based study.BMC Public Health. 2022 Sep 5;22(1):1676. doi: 10.1186/s12889-022-13918-y. BMC Public Health. 2022. PMID: 36064368 Free PMC article.
References
-
- Deeks JJ, Dinnes J, Takwoingi Y, Davenport C, Spijker R, Taylor-Phillips S, Adriano A, Beese S, Dretzke J, Ferrante di Ruffano L, Harris IM, Price MJ, Dittrich S, Emperador D, Hooft L, Leeflang MMG, Van den Bruel A, Cochrane COVID-19 Diagnostic Test Accuracy Group . 2020. Antibody tests for identification of current and past infection with SARS-CoV-2. Cochrane Database Syst Rev 6:CD013652. doi:10.1002/14651858.CD013652. - DOI - PMC - PubMed
-
- Emmerich P, Murawski C, Ehmen C, von Possel R, Pekarek N, Oestereich L, Duraffour S, Pahlmann M, Struck N, Eibach D, Krumkamp R, Amuasi J, Maiga‐Ascofaré O, Rakotozandrindrainy R, Asogun D, Ighodalo Y, Kann S, May J, Tannich E, Deschermeier C. 2021. Limited specificity of commercially available SARS-CoV-2 IgG ELISAs in serum samples of African origin. Trop Med Int Health 26:621–631. doi:10.1111/tmi.13569. - DOI - PMC - PubMed
-
- Nkuba Ndaye A, Hoxha A, Madinga J, Marien J, Peeters M, Leendertz FH, Ahuka Mundeke S, Arien KK, Muyembe Tanfumu J-J, Mbala Kingebeni P, Vanlerberghe V. 2021. Challenges in interpreting SARS-CoV-2 serological results in African countries. Lancet Glob Health 9:e588–e589. doi:10.1016/S2214-109X(21)00060-7. - DOI - PMC - PubMed
-
- Yadouleton A, Sander A-L, Moreira-Soto A, Tchibozo C, Hounkanrin G, Badou Y, Fischer C, Krause N, Akogbeto P, de Oliveira Filho EF, Dossou A, Brunink S, Aissi MAJ, Djingarey MH, Hounkpatin B, Nagel M, Drexler JF. 2021. Limited specificity of serologic tests for SARS-CoV-2 antibody detection, Benin. Emerg Infect Dis 27:233–237. doi:10.3201/eid2701.203281. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
