

Association of Prior BNT162b2 COVID-19 Vaccination With Symptomatic SARS-CoV-2 Infection in Children and Adolescents During Omicron Predominance
- PMID: 35560036
- PMCID: PMC9107063
- DOI: 10.1001/jama.2022.7493
Association of Prior BNT162b2 COVID-19 Vaccination With Symptomatic SARS-CoV-2 Infection in Children and Adolescents During Omicron Predominance
Abstract
Importance: Efficacy of 2 doses of the BNT162b2 COVID-19 vaccine (Pfizer-BioNTech) against COVID-19 was high in pediatric trials conducted before the SARS-CoV-2 Omicron variant emerged. Among adults, estimated vaccine effectiveness (VE) of 2 BNT162b2 doses against symptomatic Omicron infection was reduced compared with prior variants, waned rapidly, and increased with a booster.
Objective: To evaluate the association of symptomatic infection with prior vaccination with BNT162b2 to estimate VE among children and adolescents during Omicron variant predominance.
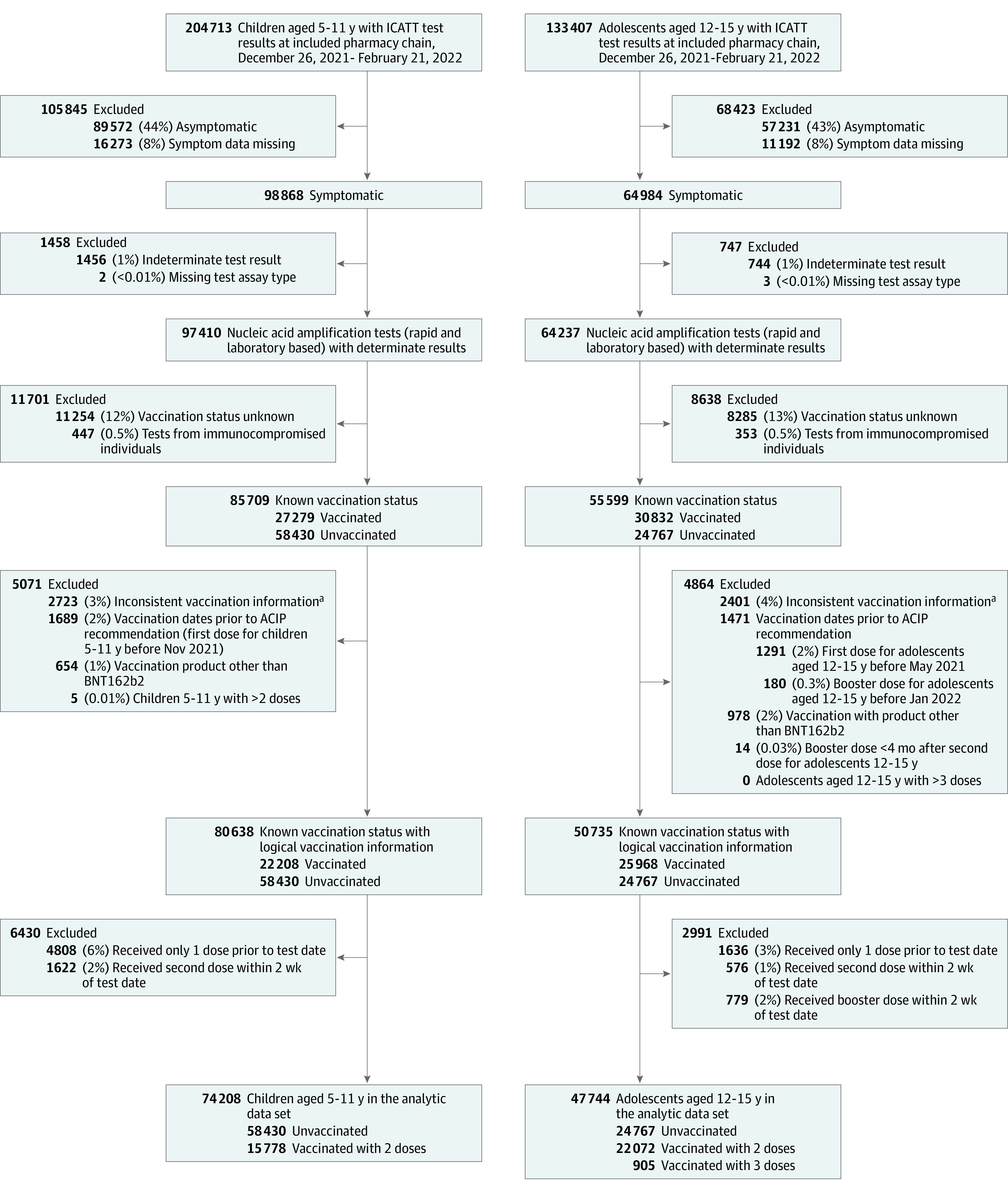
Design, setting, and participants: A test-negative, case-control analysis was conducted using data from 6897 pharmacy-based, drive-through SARS-CoV-2 testing sites across the US from a single pharmacy chain in the Increasing Community Access to Testing platform. This analysis included 74 208 tests from children 5 to 11 years of age and 47 744 tests from adolescents 12 to 15 years of age with COVID-19-like illness who underwent SARS-CoV-2 nucleic acid amplification testing from December 26, 2021, to February 21, 2022.
Exposures: Two BNT162b2 doses 2 weeks or more before SARS-CoV-2 testing vs no vaccination for children; 2 or 3 doses 2 weeks or more before testing vs no vaccination for adolescents (who are recommended to receive a booster dose).
Main outcomes and measures: Symptomatic infection. The adjusted odds ratio (OR) for the association of prior vaccination and symptomatic SARS-CoV-2 infection was used to estimate VE: VE = (1 - OR) × 100%.
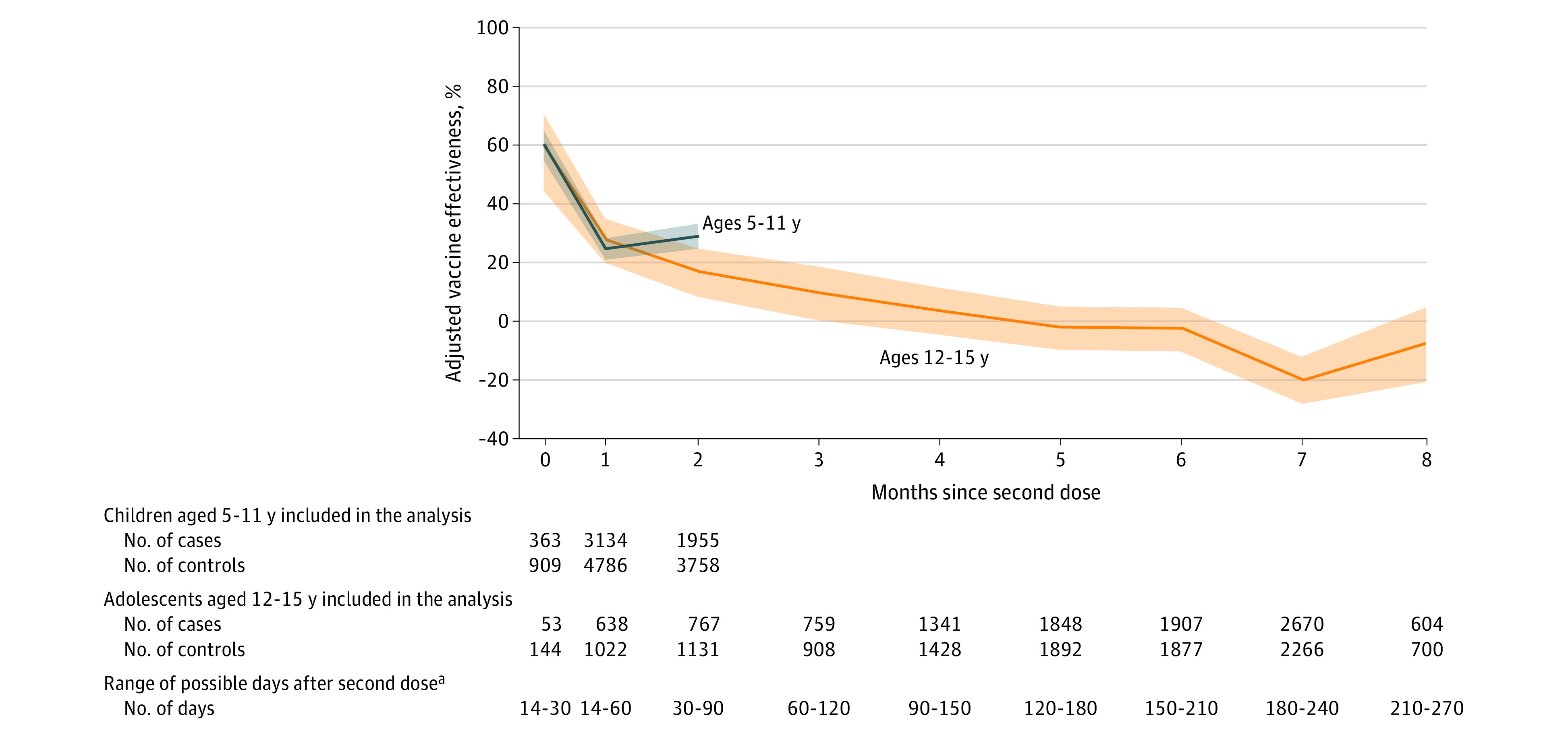
Results: A total of 30 999 test-positive cases and 43 209 test-negative controls were included from children 5 to 11 years of age, as well as 22 273 test-positive cases and 25 471 test-negative controls from adolescents 12 to 15 years of age. The median age among those with included tests was 10 years (IQR, 7-13); 61 189 (50.2%) were female, 75 758 (70.1%) were White, and 29 034 (25.7%) were Hispanic/Latino. At 2 to 4 weeks after dose 2, among children, the adjusted OR was 0.40 (95% CI, 0.35-0.45; estimated VE, 60.1% [95% CI, 54.7%-64.8%]) and among adolescents, the OR was 0.40 (95% CI, 0.29-0.56; estimated VE, 59.5% [95% CI, 44.3%-70.6%]). During month 2 after dose 2, among children, the OR was 0.71 (95% CI, 0.67-0.76; estimated VE, 28.9% [95% CI, 24.5%-33.1%]) and among adolescents, the OR was 0.83 (95% CI, 0.76-0.92; estimated VE, 16.6% [95% CI, 8.1%-24.3%]). Among adolescents, the booster dose OR 2 to 6.5 weeks after the dose was 0.29 (95% CI, 0.24-0.35; estimated VE, 71.1% [95% CI, 65.5%-75.7%]).
Conclusions and relevance: Among children and adolescents, estimated VE for 2 doses of BNT162b2 against symptomatic infection was modest and decreased rapidly. Among adolescents, the estimated effectiveness increased after a booster dose.
Conflict of interest statement
Figures
Comment in
-
Protecting Children Against Omicron.JAMA. 2022 Jun 14;327(22):2195-2197. doi: 10.1001/jama.2022.7315. JAMA. 2022. PMID: 35560309 No abstract available.
Similar articles
-
Estimated BNT162b2 Vaccine Effectiveness Against Infection With Delta and Omicron Variants Among US Children 5 to 11 Years of Age.JAMA Netw Open. 2022 Dec 1;5(12):e2246915. doi: 10.1001/jamanetworkopen.2022.46915. JAMA Netw Open. 2022. PMID: 36515946 Free PMC article.
-
Association Between 3 Doses of mRNA COVID-19 Vaccine and Symptomatic Infection Caused by the SARS-CoV-2 Omicron and Delta Variants.JAMA. 2022 Feb 15;327(7):639-651. doi: 10.1001/jama.2022.0470. JAMA. 2022. PMID: 35060999 Free PMC article.
-
Effectiveness of COVID-19 Pfizer-BioNTech BNT162b2 mRNA Vaccination in Preventing COVID-19-Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Nonimmunocompromised Children and Adolescents Aged 5-17 Years - VISION Network, 10 States, April 2021-January 2022.MMWR Morb Mortal Wkly Rep. 2022 Mar 4;71(9):352-358. doi: 10.15585/mmwr.mm7109e3. MMWR Morb Mortal Wkly Rep. 2022. PMID: 35239634 Free PMC article.
-
Effectiveness of COVID-19 Pfizer-BioNTech (BNT162b2) mRNA vaccination in adolescents aged 12-17 years: A systematic review and meta-analysis.Hum Vaccin Immunother. 2023 Dec 31;19(1):2214495. doi: 10.1080/21645515.2023.2214495. Epub 2023 Jun 5. Hum Vaccin Immunother. 2023. PMID: 37277959 Free PMC article. Review.
-
COVID-19 Vaccine Effectiveness of Booster Doses Against Delta and Omicron Variants Over Follow-up Times Using Longitudinal Meta-analysis.J Res Health Sci. 2024 Sep 30;24(4):e00626. doi: 10.34172/jrhs.2024.161. Epub 2024 Sep 30. J Res Health Sci. 2024. PMID: 39431651 Free PMC article.
Cited by
-
Evaluating the impact of extended dosing intervals on mRNA COVID-19 vaccine effectiveness in adolescents.BMC Med. 2024 Sep 12;22(1):384. doi: 10.1186/s12916-024-03597-4. BMC Med. 2024. PMID: 39267060 Free PMC article.
-
COVID-19 vaccine update: vaccine effectiveness, SARS-CoV-2 variants, boosters, adverse effects, and immune correlates of protection.J Biomed Sci. 2022 Oct 15;29(1):82. doi: 10.1186/s12929-022-00853-8. J Biomed Sci. 2022. PMID: 36243868 Free PMC article. Review.
-
Protection of the third-dose and fourth-dose mRNA vaccines against SARS-CoV-2 Omicron subvariant: a systematic review and meta-analysis.BMJ Open. 2023 Dec 20;13(12):e076892. doi: 10.1136/bmjopen-2023-076892. BMJ Open. 2023. PMID: 38128943 Free PMC article.
-
Estimated BNT162b2 Vaccine Effectiveness Against Infection With Delta and Omicron Variants Among US Children 5 to 11 Years of Age.JAMA Netw Open. 2022 Dec 1;5(12):e2246915. doi: 10.1001/jamanetworkopen.2022.46915. JAMA Netw Open. 2022. PMID: 36515946 Free PMC article.
-
The lapse of federal COVID-19 funding: implications for health equity.Pediatr Res. 2023 Mar;93(4):745-747. doi: 10.1038/s41390-023-02487-4. Epub 2023 Jan 23. Pediatr Res. 2023. PMID: 36690748 Free PMC article. No abstract available.
References
-
- Centers for Disease Control and Prevention . COVID data tracker: COVID-19 weekly cases and deaths per 100,000 population by age, race/ethnicity, and sex. Accessed January 20, 2022. https://covid.cdc.gov/covid-data-tracker/#demographicsovertime
-
- Centers for Disease Control and Prevention . COVID data tracker: new admissions of patients with confirmed COVID-19, United States. Accessed January 20, 2022. https://covid.cdc.gov/covid-data-tracker/#new-hospital-admissions
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
