

Beyond the Golden Hour: Treating Acute Stroke in the Platinum 30 Minutes
- PMID: 35545939
- PMCID: PMC9329219
- DOI: 10.1161/STROKEAHA.121.036993
Beyond the Golden Hour: Treating Acute Stroke in the Platinum 30 Minutes
Abstract
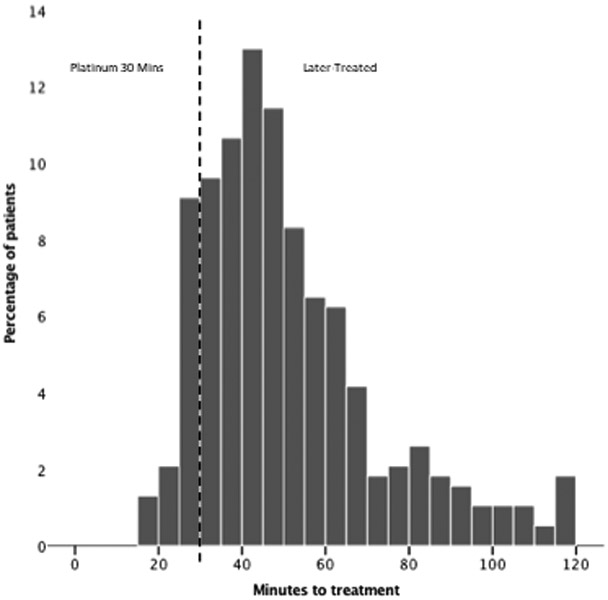
Background: To emphasize treatment speed for time-sensitive conditions, emergency medicine has developed not only the concept of the golden hour, but also the platinum half-hour. Patients with acute stroke treated within the first half-hour of onset have not been previously characterized.
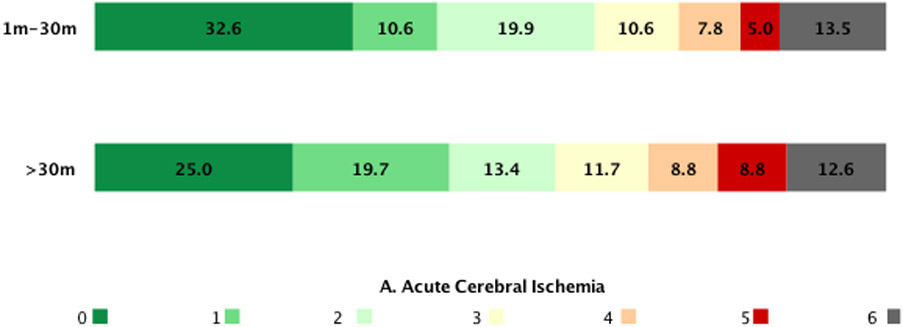
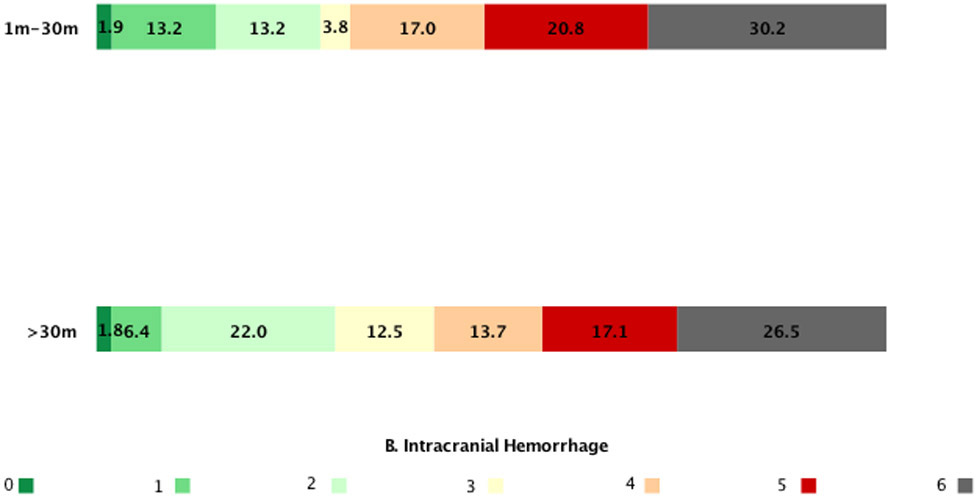
Methods: In this cohort study, we analyzed patients enrolled in the FAST-MAG (Field Administration of Stroke Therapy-Magnesium) trial, testing paramedic prehospital start of neuroprotective agent ≤2 hours of onset. The features of all acute cerebral ischemia, and intracranial hemorrhage patients with treatment starting at ≤30 m of last known well were compared with later-treated patients.
Results: Among 1680 patients, 203 (12.1%) received study agents within 30 minutes of last known well. Among platinum half-hour patients, median onset-to-treatment time was 28 minutes (interquartile range, 25-30), and final diagnoses were acute cerebral ischemia in 71.8% (ischemic stroke, 61.5%, TIA 10.3%); intracranial hemorrhage in 26.1%; and mimic in 2.5%. Clinical features among platinum half-hour patients were largely similar to later-treated patients and included age 69 (interquartile range, 57-79), 44.8% women, prehospital Los Angeles Motor Scale median 4 (3-5), and early-postarrival National Institutes of Health Stroke Scale deficit 8 (interquartile range, 3-18). Platinum half-hour acute cerebral ischemia patients did have more severe prehospital motor deficits and younger age; platinum half-hour intracranial hemorrhage patients had more severe motor deficits, were more often female, and less often of Hispanic ethnicity. Outcomes at 3 m in platinum half-hour patients were comparable to later-treated patients and included freedom-from-disability (modified Rankin Scale score, 0-1) in 35.5%, functional independence (modified Rankin Scale score, 0-2) in 53.2%, and mortality in 17.7%.
Conclusions: Prehospital initiation permits treatment start within the platinum half-hour after last known well in a substantial proportion of acute ischemic and hemorrhagic stroke patients, accounting for more than 1 in 10 enrolled in a multicenter trial. Hyperacute platinum half-hour patients were largely similar to later-treated patients and are an attainable target for treatment in prehospital stroke trials.
Keywords: blood pressure; cerebral hemorrhage; reperfusion; thrombectomy; transient ischemic attack.
Figures

Similar articles
-
Frequency, Predictors, and Outcomes of Prehospital and Early Postarrival Neurological Deterioration in Acute Stroke: Exploratory Analysis of the FAST-MAG Randomized Clinical Trial.JAMA Neurol. 2018 Nov 1;75(11):1364-1374. doi: 10.1001/jamaneurol.2018.1893. JAMA Neurol. 2018. PMID: 30039165 Free PMC article. Clinical Trial.
-
Prehospital use of magnesium sulfate as neuroprotection in acute stroke.N Engl J Med. 2015 Feb 5;372(6):528-36. doi: 10.1056/NEJMoa1408827. N Engl J Med. 2015. PMID: 25651247 Free PMC article. Clinical Trial.
-
Field Validation of the Los Angeles Motor Scale as a Tool for Paramedic Assessment of Stroke Severity.Stroke. 2017 Feb;48(2):298-306. doi: 10.1161/STROKEAHA.116.015247. Epub 2017 Jan 13. Stroke. 2017. PMID: 28087807 Clinical Trial.
-
Endovascular Treatment of Acute Ischemic Stroke Due to Tandem Occlusions: Large Multicenter Series and Systematic Review.Cerebrovasc Dis. 2016;41(5-6):306-12. doi: 10.1159/000444069. Epub 2016 Feb 17. Cerebrovasc Dis. 2016. PMID: 26881779 Review.
-
Prehospital stroke detection scales: A head-to-head comparison of 7 scales in patients with suspected stroke.Int J Stroke. 2025 Mar;20(3):268-277. doi: 10.1177/17474930241275123. Epub 2024 Sep 10. Int J Stroke. 2025. PMID: 39127910 Free PMC article. Review.
References
-
- Saver JL. Time is brain—quantified. Stroke. 2006;37:263–266. - PubMed
-
- Emberson J, Lees KR, Lyden P, Blackwell L, Albers G, Bluhmki E, Brott T, Cohen G, Davis S, Donnan G, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. The Lancet. 2014;384:929–935. - PMC - PubMed
-
- Saver JL, Fonarow GC, Smith EE, Reeves MJ, Grau-Sepulveda MV, Pan W, Olson DM, Hernandez AF, Peterson ED, Schwamm LH. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. Jama. 2013;309:480–488. - PubMed
-
- Saver JL, Goyal M, Van der Lugt AA, Menon BK, Majoie CB, Dippel DW, Campbell BC, Nogueira RG, Demchuk AM, Tomasello A, et al. Time to treatment with endovascular thrombectomy and outcomes from ischemic stroke: a meta-analysis. Jama. 2016;316:279–289. - PubMed
-
- Jahan R, Saver JL, Schwamm LH, Fonarow GC, Liang L, Matsouaka RA, Xian Y, Holmes DN, Peterson ED, Yavagal D, et al. Association between time to treatment with endovascular reperfusion therapy and outcomes in patients with acute ischemic stroke treated in clinical practice. Jama. 2019;322:252–263. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
