

Epidemiology, Drug Susceptibility, and Clinical Risk Factors in Patients With Invasive Aspergillosis
- PMID: 35493371
- PMCID: PMC9051236
- DOI: 10.3389/fpubh.2022.835092
Epidemiology, Drug Susceptibility, and Clinical Risk Factors in Patients With Invasive Aspergillosis
Abstract
Background: This study aimed to investigate the Aspergillus species distribution, antifungal sensitivities, clinical characteristics, and risk factors of patients with invasive aspergillosis (IA) in a tertiary teaching hospital in Anhui Province.
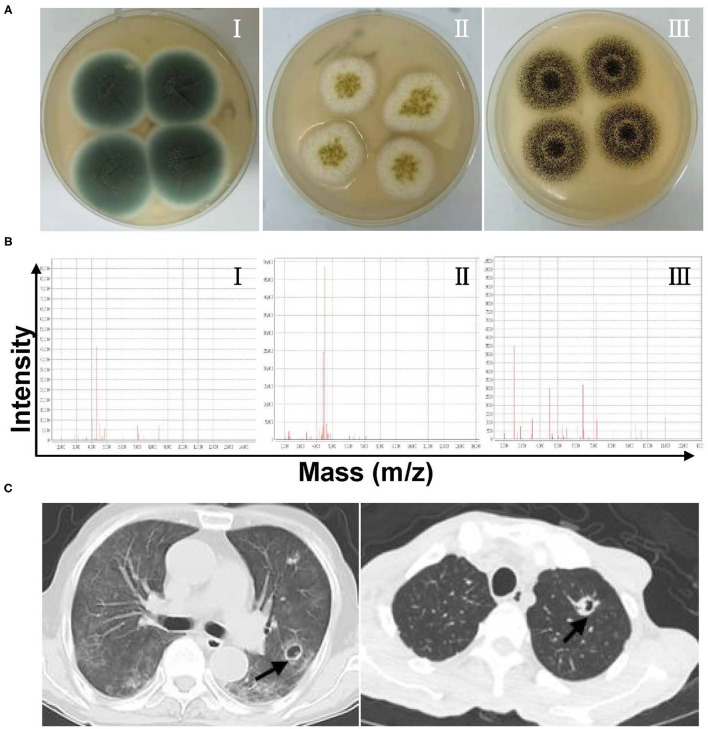
Methods: In the present study, 156 Aspergillus isolates were collected from patients admitted to a 2,800-bed comprehensive hospital between January 2019 and April 2021. The epidemiology of Aspergillus species was well-examined, and its antifungal susceptibility was specifically measured by the microbroth dilution method. The risk factors of patients with IA were documented and analyzed intensively. In addition, gene sequencing was employed to determine gene mutations of cytochrome P450 14-α sterol demethylase-Aspergillus (cyp51A) associated with azole resistance among Aspergillus fumigatus.
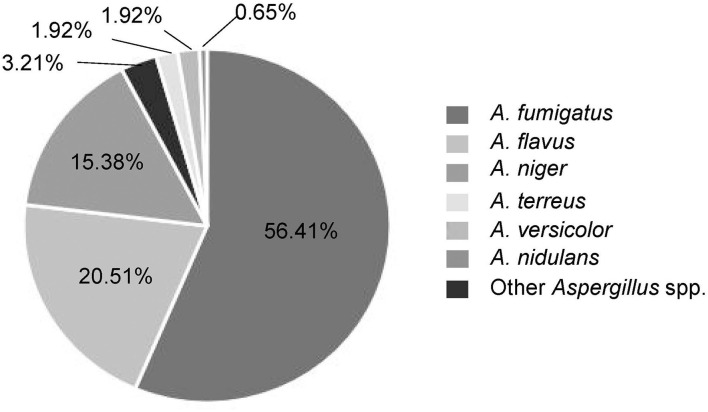
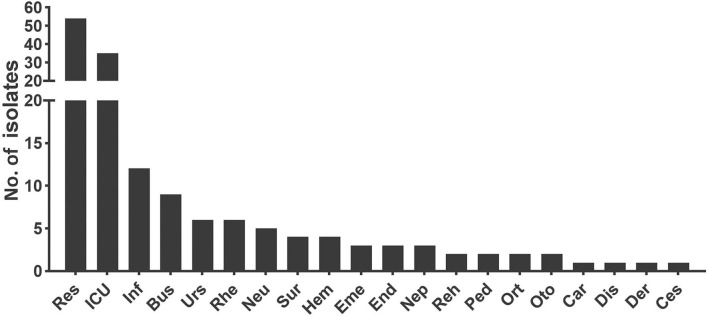
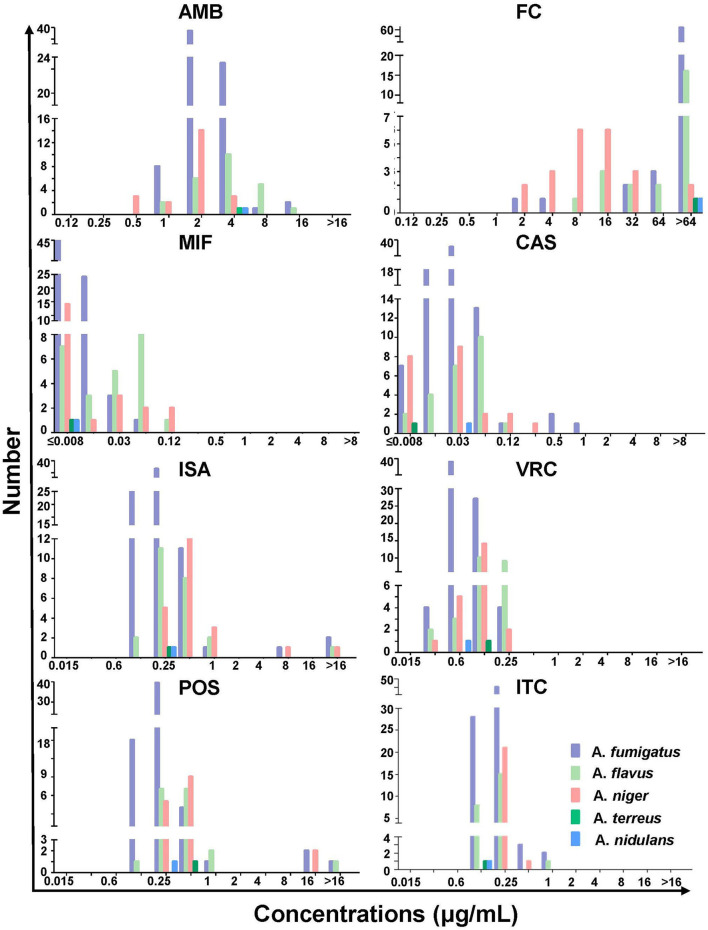
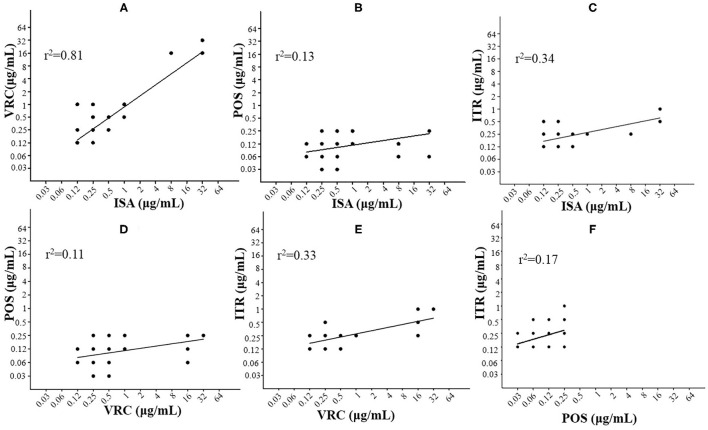
Results: The Aspergillus species distribution was dominated by A. fumigatus (56.41%), Aspergillus flavus (20.51%), and Aspergillus niger (15.38%) locally. In particular, all Aspergillus species showed very low minimum inhibitory concentrations (MICs, ≤ 0.5 μg/ml) for azoles and echinocandins, slightly high MICs (1.66-2.91 μg/ml) for amphotericin B, and exceptionally high MICs (>64 μg/ml) for flucytosine. Azole-resistant rate of Aspergillus species in this local region reached up to 5.79%. Correlation analyses of multiple antifungals indicate a significant MIC relevance between isavuconazole and voriconazole (Pearson correlation coefficient was 0.81, P < 0.0001). The clinical risk factors for patients with IA were found primarily to be pulmonary diseases (P = 0.007) and patients' age (P < 0.001). Notably, three mutant loci (TR46/Y121F/T289A) of the cyp51A gene were identified in azole-resistant A. fumigatus.
Conclusions: The Aspergillus species emerged increasingly, of which A. fumigatus and A. flavus remained the main pathogens for invasive Aspergillus infections in the local region. The vast majority of Aspergillus species exhibited good susceptibility to all the antifungals, except flucytosine. The local occurrence of azole-resistant Aspergillus species grew gradually and needed monitoring in time. Pulmonary diseases and age were likely considered as highly associated risk factors for IA. To our knowledge, the clinically isolated azole-resistant A. fumigatus with TR46/Y121F/T289A mutations identified here were rarely reported in the area of China.
Keywords: Aspergillus spp.; antifungal sensitivity; azole resistance; invasive aspergillosis; risk factors.
Copyright © 2022 Wang, Zhang, Zhou, Zhang and Xu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Aspergillosis due to voriconazole highly resistant Aspergillus fumigatus and recovery of genetically related resistant isolates from domiciles.Clin Infect Dis. 2013 Aug;57(4):513-20. doi: 10.1093/cid/cit320. Epub 2013 May 10. Clin Infect Dis. 2013. PMID: 23667263
-
Azole, polyene and echinocandin MIC distributions for wild-type, TR34/L98H and TR46/Y121F/T289A Aspergillus fumigatus isolates in the Netherlands.J Antimicrob Chemother. 2015 Jan;70(1):178-81. doi: 10.1093/jac/dku364. Epub 2014 Oct 9. J Antimicrob Chemother. 2015. PMID: 25301884
-
First azole-resistant Aspergillus fumigatus isolates with the environmental TR46 /Y121F/T289A mutation in Iran.Mycoses. 2020 May;63(5):430-436. doi: 10.1111/myc.13064. Epub 2020 Mar 13. Mycoses. 2020. PMID: 32056319 Free PMC article.
-
Azole-resistant Aspergillus fumigatus: A global phenomenon originating in the environment?Med Mal Infect. 2020 Aug;50(5):389-395. doi: 10.1016/j.medmal.2019.07.014. Epub 2019 Aug 28. Med Mal Infect. 2020. PMID: 31472992 Review.
-
Clinical implications of globally emerging azole resistance in Aspergillus fumigatus.Philos Trans R Soc Lond B Biol Sci. 2016 Dec 5;371(1709):20150460. doi: 10.1098/rstb.2015.0460. Philos Trans R Soc Lond B Biol Sci. 2016. PMID: 28080986 Free PMC article. Review.
Cited by
-
Dual use of antifungals in medicine and agriculture: How do we help prevent resistance developing in human pathogens?Drug Resist Updat. 2022 Dec;65:100885. doi: 10.1016/j.drup.2022.100885. Epub 2022 Oct 20. Drug Resist Updat. 2022. PMID: 36283187 Free PMC article.
-
Antifungal Susceptibility and Genotypic Analysis of cyp51A Mutations in Aspergillus fumigatus Isolates in Malaysia.Infect Drug Resist. 2024 May 29;17:2159-2168. doi: 10.2147/IDR.S452619. eCollection 2024. Infect Drug Resist. 2024. PMID: 38828376 Free PMC article.
-
Epidemiology and Azole Resistance of Clinical Isolates of Aspergillus fumigatus from a Large Tertiary Hospital in Ningxia, China.Infect Drug Resist. 2024 Feb 2;17:427-439. doi: 10.2147/IDR.S440363. eCollection 2024. Infect Drug Resist. 2024. PMID: 38328338 Free PMC article.
-
Distribution of Aspergillus species and risk factors for aspergillosis in mainland China: a systematic review.Ther Adv Infect Dis. 2024 Jun 4;11:20499361241252537. doi: 10.1177/20499361241252537. eCollection 2024 Jan-Dec. Ther Adv Infect Dis. 2024. PMID: 38835831 Free PMC article. Review.
-
Loss of the mammalian G-protein coupled receptor, G2A, modulates severity of invasive pulmonary aspergillosis.Front Immunol. 2023 Jun 26;14:1173544. doi: 10.3389/fimmu.2023.1173544. eCollection 2023. Front Immunol. 2023. PMID: 37435068 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous