

Analgesic Outcomes in Opioid Use Disorder Patients Receiving Spinal Anesthesia with or without Intrathecal Clonidine for Cesarean Delivery: A Retrospective Investigation
- PMID: 35478995
- PMCID: PMC9037861
- DOI: 10.2147/JPR.S358045
Analgesic Outcomes in Opioid Use Disorder Patients Receiving Spinal Anesthesia with or without Intrathecal Clonidine for Cesarean Delivery: A Retrospective Investigation
Abstract
Background: Intrathecal (IT) clonidine has been observed to reduce 24-hour opioid requirements and time to first analgesic request after cesarean delivery, but has not been specifically studied in patients with opioid use disorder (OUD).
Methods: Patients with OUD undergoing cesarean delivery under spinal or combined spinal-epidural (CSE) anesthesia at our institution from 2011 to 2020 were identified, and only patients with OUD were included in this study. Subjects that received IT clonidine were compared to a control group that did not receive IT clonidine to observe potential differences in analgesic outcomes (24-hour opioid requirements, pain scores and time to first post-operative pain medication) or side-effects (hypotension, vasopressor dosing and bradycardia).
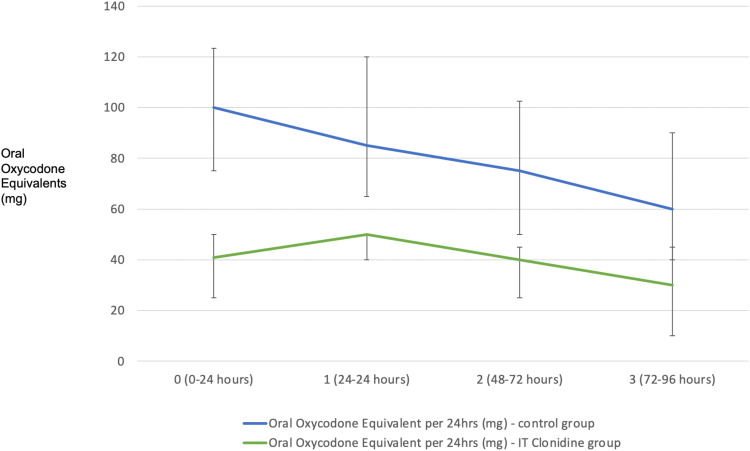
Results: A total of 160 patients were included (clonidine n = 22, controls n = 138). For the clonidine group, the median IT clonidine dose was 30µg. Clonidine group patients were observed to have greater dose of IT bupivacaine (12 vs 12.75mg; p = 0.01) and IT morphine (100 vs 200µg; p < 0.001). The clonidine group was also observed to have greater incidence of intraoperative hypotension (20% vs 45%; p = 0.01) and maximum phenylephrine dose (50 vs 57.5 µg/min; p < 0.001). The time to first analgesic request (minutes) after surgery was significantly longer for the clonidine group (153.5 vs 207 min; p < 0.001). The average oral oxycodone equivalents taken per 24 hours of hospital admission were significantly less in the clonidine group (82.36 vs 41.67mg; p < 0.001), and the clonidine group also had significantly less oxycodone equivalents taken for each post-operative day.
Conclusion: IT clonidine was observed to result in reduced 24-hour opioid consumption in patients with OUD and may be useful as part of a multimodal analgesic regimen. The incidence of hypotension and vasopressor doses were greater in patients receiving IT clonidine, and this should be anticipated if IT clonidine is being administered.
Keywords: cesarean analgesia; clonidine; enhanced recovery; opioid use disorder.
© 2022 Cook et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Post-Cesarean Delivery Analgesic Outcomes in Patients Maintained on Methadone and Buprenorphine: A Retrospective Investigation.J Pain Res. 2020 Dec 30;13:3513-3524. doi: 10.2147/JPR.S284874. eCollection 2020. J Pain Res. 2020. PMID: 33408510 Free PMC article.
-
An evaluation of the postoperative antihyperalgesic and analgesic effects of intrathecal clonidine administered during elective cesarean delivery.Anesth Analg. 2008 Sep;107(3):948-55. doi: 10.1213/ane.0b013e31817f1595. Anesth Analg. 2008. PMID: 18713912 Clinical Trial.
-
Hemodynamic and analgesic profile after intrathecal clonidine in humans. A dose-response study.Anesthesiology. 1994 Sep;81(3):591-601; discussion 27A-28A. doi: 10.1097/00000542-199409000-00011. Anesthesiology. 1994. PMID: 8092504 Clinical Trial.
-
Comparison of postoperative analgesic effect of intrathecal clonidine and fentanyl added to bupivacaine in patients undergoing cesarean section: a prospective randomized double-blind study.Pain Res Treat. 2014;2014:513628. doi: 10.1155/2014/513628. Epub 2014 Feb 4. Pain Res Treat. 2014. PMID: 24649361 Free PMC article.
-
The Effect of Intrathecal Morphine Dose on Outcomes After Elective Cesarean Delivery: A Meta-Analysis.Anesth Analg. 2016 Jul;123(1):154-64. doi: 10.1213/ANE.0000000000001255. Anesth Analg. 2016. PMID: 27089000 Review.
Cited by
-
Neuraxial clonidine is not associated with lower post-cesarean opioid consumption or pain scores in parturients on chronic buprenorphine therapy: a retrospective cohort study.J Anesth. 2024 Jun;38(3):339-346. doi: 10.1007/s00540-024-03314-8. Epub 2024 Mar 10. J Anesth. 2024. PMID: 38461452
-
Developing non-opioid therapeutics to alleviate pain among persons with opioid use disorder: a review of the human evidence.Int Rev Psychiatry. 2023 Aug-Sep;35(5-6):377-396. doi: 10.1080/09540261.2023.2229430. Epub 2023 Jun 28. Int Rev Psychiatry. 2023. PMID: 38299655 Free PMC article. Review.
References
-
- Maeda A, Bateman BT, Clancy CR, Creanga AA, Leffert LR. Opioid abuse and dependence during pregnancy: temporal trends and obstetrical outcomes. J Am Soc Anesthesiol. 2014;121(6):1158–1165. - PubMed
LinkOut - more resources
Full Text Sources
