

Engineered cellular immunotherapies in cancer and beyond
- PMID: 35440724
- PMCID: PMC9305718
- DOI: 10.1038/s41591-022-01765-8
Engineered cellular immunotherapies in cancer and beyond
Abstract
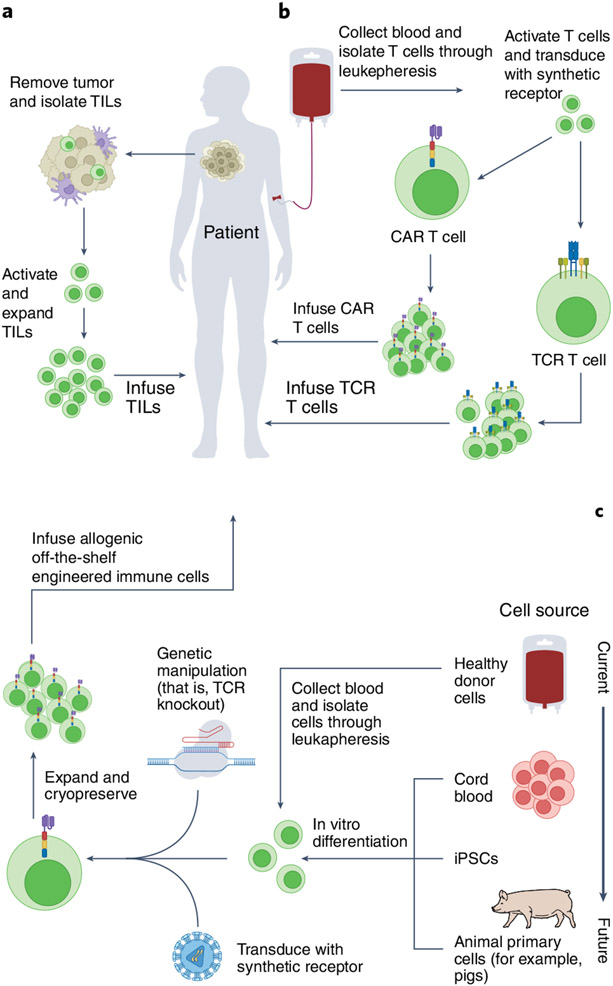
This year marks the tenth anniversary of cell therapy with chimeric antigen receptor (CAR)-modified T cells for refractory leukemia. The widespread commercial approval of genetically engineered T cells for a variety of blood cancers offers hope for patients with other types of cancer, and the convergence of human genome engineering and cell therapy technology holds great potential for generation of a new class of cellular therapeutics. In this Review, we discuss the goals of cellular immunotherapy in cancer, key challenges facing the field and exciting strategies that are emerging to overcome these obstacles. Finally, we outline how developments in the cancer field are paving the way for cellular immunotherapeutics in other diseases.
© 2022. Springer Nature America, Inc.
Figures
Similar articles
-
Generation of CAR-T Cells for Cancer Immunotherapy.Methods Mol Biol. 2019;1884:349-360. doi: 10.1007/978-1-4939-8885-3_24. Methods Mol Biol. 2019. PMID: 30465215
-
From antibodies to living drugs: Quo vadis cancer immunotherapy?Biol Futur. 2021 Mar;72(1):85-99. doi: 10.1007/s42977-021-00072-6. Epub 2021 Feb 1. Biol Futur. 2021. PMID: 34554498 Review.
-
CRISPR/Cas9 and CAR-T cell, collaboration of two revolutionary technologies in cancer immunotherapy, an instruction for successful cancer treatment.Hum Immunol. 2018 Dec;79(12):876-882. doi: 10.1016/j.humimm.2018.09.007. Epub 2018 Sep 24. Hum Immunol. 2018. PMID: 30261221 Review.
-
Prospects and challenges for use of CAR T cell therapies in solid tumors.Expert Opin Biol Ther. 2020 May;20(5):503-516. doi: 10.1080/14712598.2020.1738378. Epub 2020 Mar 12. Expert Opin Biol Ther. 2020. PMID: 32125191 Review.
-
Next-generation CAR T cells to overcome current drawbacks.Int J Hematol. 2021 Nov;114(5):532-543. doi: 10.1007/s12185-020-02923-9. Epub 2020 Jun 27. Int J Hematol. 2021. PMID: 32594314 Review.
Cited by
-
Convergent inducers and effectors of T cell paralysis in the tumour microenvironment.Nat Rev Cancer. 2025 Jan;25(1):41-58. doi: 10.1038/s41568-024-00761-z. Epub 2024 Oct 24. Nat Rev Cancer. 2025. PMID: 39448877 Review.
-
Genetically Engineered Macrophages Co-Loaded with CD47 Inhibitors Synergistically Reconstruct Efferocytosis and Improve Cardiac Remodeling Post Myocardial Ischemia Reperfusion Injury.Adv Healthc Mater. 2024 Jun;13(16):e2303267. doi: 10.1002/adhm.202303267. Epub 2024 Mar 13. Adv Healthc Mater. 2024. PMID: 38198534 Free PMC article.
-
Adenovirus vaccine targeting kinases induces potent antitumor immunity in solid tumors.J Immunother Cancer. 2024 Aug 28;12(8):e009869. doi: 10.1136/jitc-2024-009869. J Immunother Cancer. 2024. PMID: 39209449 Free PMC article.
-
Adenoviral vectors infect B lymphocytes in vivo.Mol Ther. 2023 Sep 6;31(9):2600-2611. doi: 10.1016/j.ymthe.2023.07.004. Epub 2023 Jul 14. Mol Ther. 2023. PMID: 37452494 Free PMC article.
-
Breast cancer clinical outcomes and tumor immune microenvironment: cross-dialogue of multiple epigenetic modification profiles.Aging (Albany NY). 2024 May 22;16(10):8998-9022. doi: 10.18632/aging.205853. Epub 2024 May 22. Aging (Albany NY). 2024. PMID: 38796789 Free PMC article.
References
-
- Combination Products (FDA, accessed 1 March 2022); https://www.fda.gov/combination-products
-
- Frangoul H et al. CRISPR–Cas9 gene editing for sickle cell disease and β-thalassemia. N. Engl. J. Med 384, 252–260 (2021). - PubMed
-
- Approved Cellular and Gene Therapy (FDA, 2022); https://www.fda.gov/vaccines-blood-biologics/cellular-gene-therapy-produ...
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
