

Lipids in Liver Failure Syndromes: A Focus on Eicosanoids, Specialized Pro-Resolving Lipid Mediators and Lysophospholipids
- PMID: 35432367
- PMCID: PMC9008479
- DOI: 10.3389/fimmu.2022.867261
Lipids in Liver Failure Syndromes: A Focus on Eicosanoids, Specialized Pro-Resolving Lipid Mediators and Lysophospholipids
Abstract
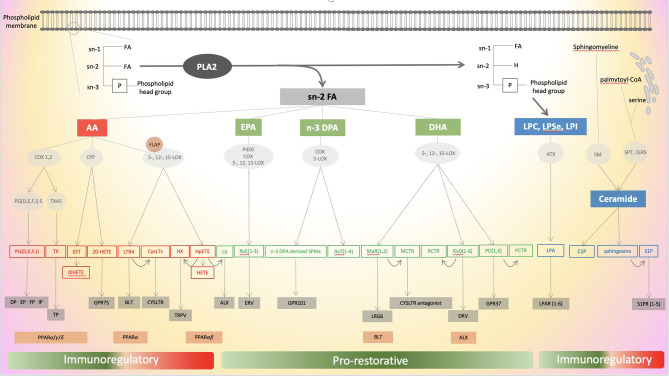
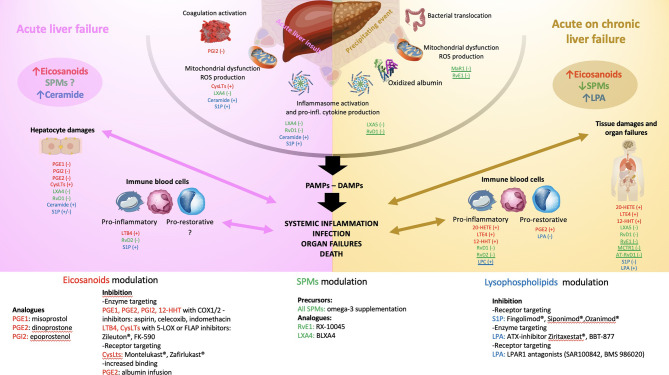
Lipids are organic compounds insoluble in water with a variety of metabolic and non-metabolic functions. They not only represent an efficient energy substrate but can also act as key inflammatory and anti-inflammatory molecules as part of a network of soluble mediators at the interface of metabolism and the immune system. The role of endogenous bioactive lipid mediators has been demonstrated in several inflammatory diseases (rheumatoid arthritis, inflammatory bowel disease, atherosclerosis, cancer). The liver is unique in providing balanced immunotolerance to the exposure of bacterial components from the gut transiting through the portal vein and the lymphatic system. This balance is abruptly deranged in liver failure syndromes such as acute liver failure and acute-on-chronic liver failure. In these syndromes, researchers have recently focused on bioactive lipid mediators by global metabonomic profiling and uncovered the pivotal role of these mediators in the immune dysfunction observed in liver failure syndromes explaining the high occurrence of sepsis and subsequent organ failure. Among endogenous bioactive lipids, the mechanistic actions of three classes (eicosanoids, pro-resolving lipid mediators and lysophospholipids) in the pathophysiological modulation of liver failure syndromes will be the topic of this narrative review. Furthermore, the therapeutic potential of lipid-immune pathways will be described.
Keywords: acute liver failure; acute on chronic liver failure; cirrhosis; lipids; liver; liver failure; metabonome; systems biology.
Copyright © 2022 Artru, McPhail, Triantafyllou and Trovato.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Bioactive Lipids and Chronic Inflammation: Managing the Fire Within.Front Immunol. 2018 Jan 29;9:38. doi: 10.3389/fimmu.2018.00038. eCollection 2018. Front Immunol. 2018. PMID: 29434586 Free PMC article. Review.
-
Bioactive lipids, inflammation and chronic diseases.Adv Drug Deliv Rev. 2020;159:133-169. doi: 10.1016/j.addr.2020.06.028. Epub 2020 Jul 3. Adv Drug Deliv Rev. 2020. PMID: 32628989 Review.
-
Emerging Role of Phospholipase-Derived Cleavage Products in Regulating Eosinophil Activity: Focus on Lysophospholipids, Polyunsaturated Fatty Acids and Eicosanoids.Int J Mol Sci. 2021 Apr 21;22(9):4356. doi: 10.3390/ijms22094356. Int J Mol Sci. 2021. PMID: 33919453 Free PMC article. Review.
-
Impact of Androgens on Inflammation-Related Lipid Mediator Biosynthesis in Innate Immune Cells.Front Immunol. 2020 Jun 30;11:1356. doi: 10.3389/fimmu.2020.01356. eCollection 2020. Front Immunol. 2020. PMID: 32714332 Free PMC article. Review.
-
Emerging roles of pro-resolving lipid mediators in immunological and adaptive responses to exercise-induced muscle injury.Exerc Immunol Rev. 2016;22:110-34. Exerc Immunol Rev. 2016. PMID: 26853678 Review.
Cited by
-
Metabolic Dysregulation and Metabolite Imbalances in Acute-on-chronic Liver Failure: Impact on Immune Status.J Clin Transl Hepatol. 2024 Oct 28;12(10):865-877. doi: 10.14218/JCTH.2024.00203. Epub 2024 Sep 19. J Clin Transl Hepatol. 2024. PMID: 39440217 Free PMC article. Review.
-
TLCD1 and TLCD2 regulate cellular phosphatidylethanolamine composition and promote the progression of non-alcoholic steatohepatitis.Nat Commun. 2022 Oct 14;13(1):6020. doi: 10.1038/s41467-022-33735-6. Nat Commun. 2022. PMID: 36241646 Free PMC article.
-
The Impact of Liver Failure on the Immune System.Int J Mol Sci. 2024 Sep 1;25(17):9522. doi: 10.3390/ijms25179522. Int J Mol Sci. 2024. PMID: 39273468 Free PMC article. Review.
-
Role of Oxylipins in the Inflammatory-Related Diseases NAFLD, Obesity, and Type 2 Diabetes.Metabolites. 2022 Dec 9;12(12):1238. doi: 10.3390/metabo12121238. Metabolites. 2022. PMID: 36557276 Free PMC article. Review.
References
-
- Chevreul ME, Dijkstra AJ, List GR, Wisniak J. A Chemical Study of Oils and Fats of Animal Origin. In: Sàrl Dijkstra-Tucker Carbougnères. St Eutrope-de-Born: Sàrl Dijkstra-Tucker Carbougnères; (2009). Available at: https://books.google.fr/books?id=cJovQAAACAAJ.
-
- Keys A. Seven Countries: A Multivariate Analysis of Death and Coronary Heart Disease. Cambridge, MA and London, England: Harvard University Press; (1980). doi: 10.4159/harvard.9780674497887 - DOI
-
- Majno G, Joris I. Cells, Tissues, and Disease: Principles of General Pathology. New York: Oxford University Press; (2004). Available at: https://books.google.fr/books?id=8yAf6U7njlcC.
-
- Kumar V, Abbas AK, Aster JC. Robbins and Cotran Pathologic Basis of Disease, Professional Edition E-Book. Philadelphia: Elsevier Health Sciences; (2014). Available at: https://books.google.fr/books?id=5NbsAwAAQBAJ.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources