

Neutrophilic Asthma Is Associated With Smoking, High Numbers of IRF5+, and Low Numbers of IL10+ Macrophages
- PMID: 35387061
- PMCID: PMC8974785
- DOI: 10.3389/falgy.2021.676930
Neutrophilic Asthma Is Associated With Smoking, High Numbers of IRF5+, and Low Numbers of IL10+ Macrophages
Abstract
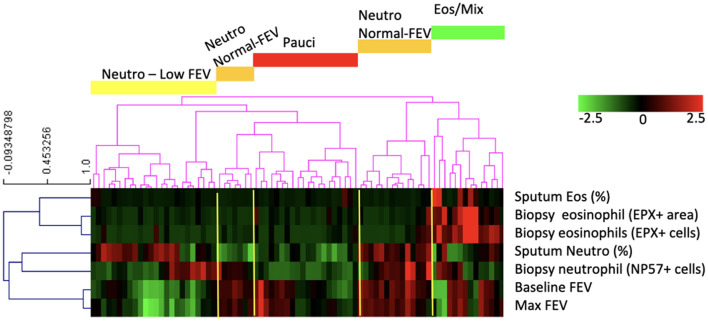
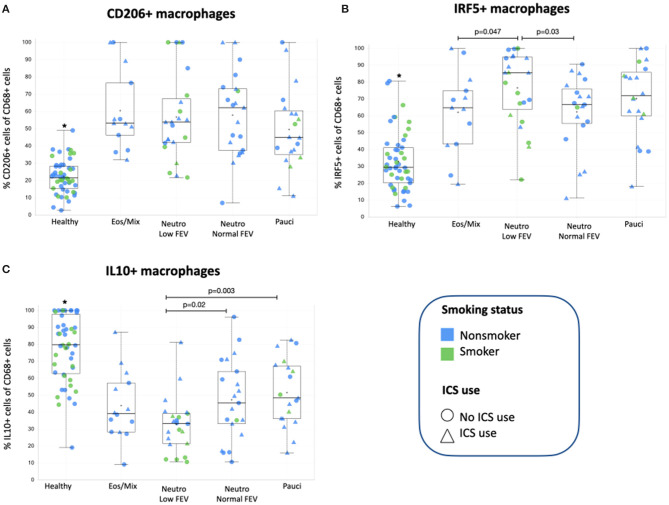
Asthma is a heterogenous disease with different inflammatory subgroups that differ in disease severity. This disease variation is hampering treatment and development of new treatment strategies. Macrophages may contribute to asthma phenotypes by their ability to activate in different ways, i.e., T helper cell 1 (Th1)-associated, Th2-associated, or anti-inflammatory activation. It is currently unknown if these different types of activation correspond with specific inflammatory subgroups of asthma. We hypothesized that eosinophilic asthma would be characterized by having Th2-associated macrophages, whereas neutrophilic asthma would have Th1-associated macrophages and both having few anti-inflammatory macrophages. We quantified macrophage subsets in bronchial biopsies of asthma patients using interferon regulatory factor 5 (IRF5)/CD68 for Th1-associated macrophages, CD206/CD68 for Th2-associated macrophages and interleukin 10 (IL10)/CD68 for anti-inflammatory macrophages. Macrophage subset percentages were investigated in subgroups of asthma as defined by unsupervised clustering using neutrophil/eosinophil counts in sputum and tissue and forced expiratory volume in 1 s (FEV1). Asthma patients clustered into four subgroups: mixed-eosinophilic/neutrophilic, paucigranulocytic, neutrophilic with normal FEV1, and neutrophilic with low FEV1, the latter group consisting mainly of smokers. No differences were found for CD206+ macrophages within asthma subgroups. In contrast, IRF5+ macrophages were significantly higher and IL10+ macrophages lower in neutrophilic asthmatics with low FEV1 as compared to those with neutrophilic asthma and normal FEV1 or mixed-eosinophilic asthma. This study shows that neutrophilic asthma with low FEV1 is associated with high numbers of IRF5+, and low numbers of IL10+ macrophages, which may be the result of combined effects of smoking and having asthma.
Keywords: CD206; FEV1; M1; M2; biopsy; inflammatory endotypes; macrophages subtypes.
Copyright © 2021 Turan, van der Veen, Draijer, Fattahi, ten Hacken, Timens, van Oosterhout, van den Berge and Melgert.
Conflict of interest statement
AO and NT were employed by the company GlaxoSmithKline at the time of data analysis and manuscript writing. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Neutrophilic asthma features increased airway classical monocytes.Clin Exp Allergy. 2021 Feb;51(2):305-317. doi: 10.1111/cea.13811. Epub 2021 Jan 1. Clin Exp Allergy. 2021. PMID: 33301598
-
Elevated serum IgE, oral corticosteroid dependence and IL-17/22 expression in highly neutrophilic asthma.Eur Respir J. 2019 Nov 7;54(5):1900068. doi: 10.1183/13993003.00068-2019. Print 2019 Nov. Eur Respir J. 2019. PMID: 31439682
-
Detailed analysis of sputum and systemic inflammation in asthma phenotypes: are paucigranulocytic asthmatics really non-inflammatory?BMC Pulm Med. 2016 Apr 5;16:46. doi: 10.1186/s12890-016-0208-2. BMC Pulm Med. 2016. PMID: 27044366 Free PMC article.
-
The onset, development and pathogenesis of severe neutrophilic asthma.Immunol Cell Biol. 2022 Mar;100(3):144-159. doi: 10.1111/imcb.12522. Epub 2022 Feb 16. Immunol Cell Biol. 2022. PMID: 35080788 Review.
-
Neutrophils and Asthma.Diagnostics (Basel). 2022 May 8;12(5):1175. doi: 10.3390/diagnostics12051175. Diagnostics (Basel). 2022. PMID: 35626330 Free PMC article. Review.
Cited by
-
ST2-Mediated Neutrophilic Airway Inflammation: A Therapeutic Target for Patients With Uncontrolled Asthma.Allergy Asthma Immunol Res. 2024 Jan;16(1):22-41. doi: 10.4168/aair.2024.16.1.22. Allergy Asthma Immunol Res. 2024. PMID: 38262389 Free PMC article.
-
Pre-asthma: a useful concept? A EUFOREA paper. Part 2-late onset eosinophilic asthma.Front Allergy. 2024 May 15;5:1404735. doi: 10.3389/falgy.2024.1404735. eCollection 2024. Front Allergy. 2024. PMID: 38812719 Free PMC article. Review.
References
LinkOut - more resources
Full Text Sources