

Pediatric vascular anomalies with airway compromise
- PMID: 35347777
- PMCID: PMC10084185
- DOI: 10.1111/jop.13297
Pediatric vascular anomalies with airway compromise
Abstract
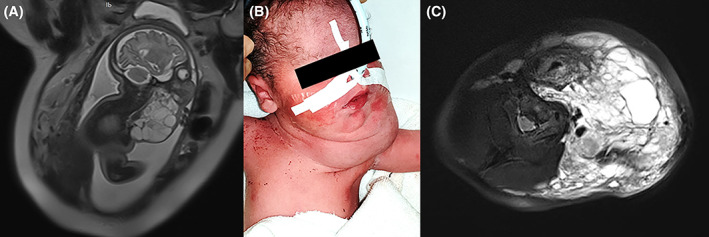
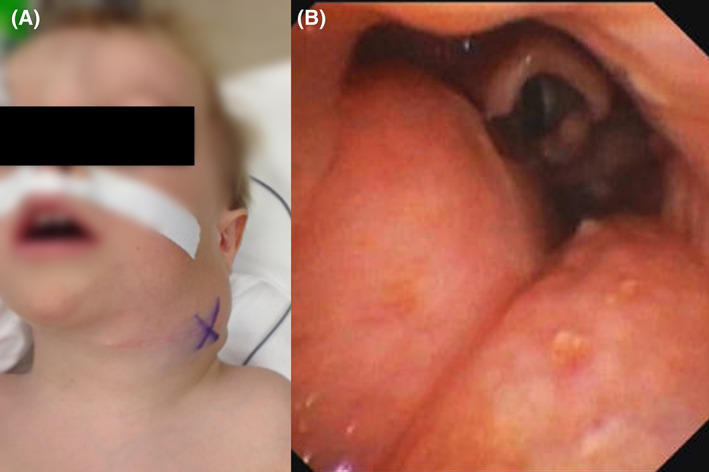
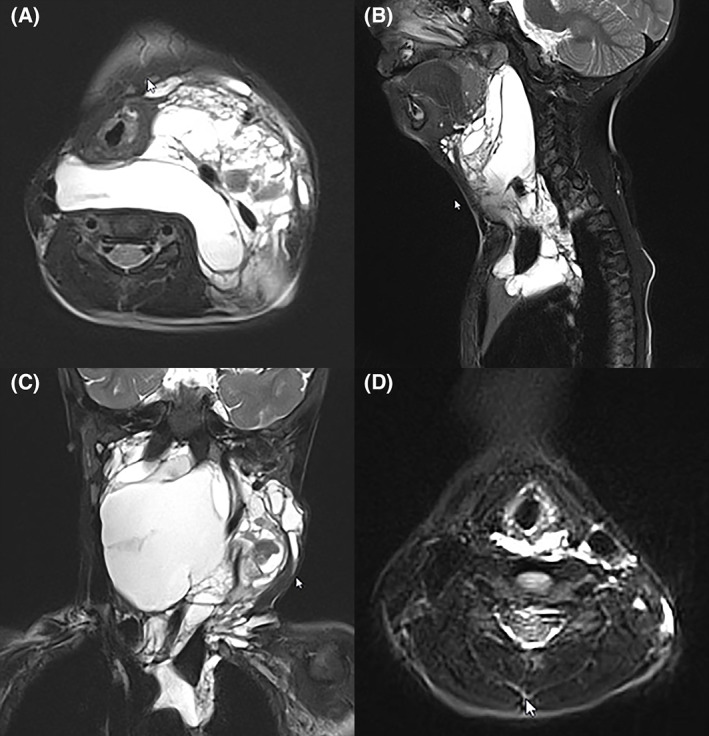
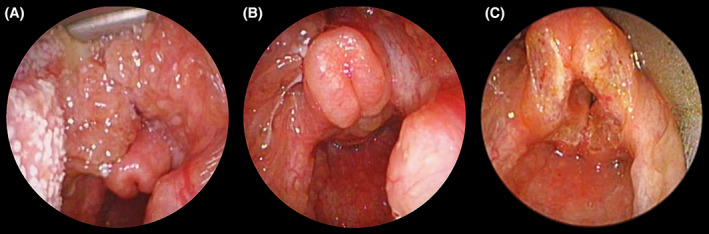
Vascular anomalies are rare lesions of diverse nature that may affect the head and neck region. Any mass in or around the upper airway has the potential to obstruct or compromise it. The absolute priority, before etiologic treatment, is the evaluation of the risk for the airway and its management. Prenatal diagnosis of an upper airway obstruction requires a planned delivery in a center having a specialized team experienced in managing a compromised feto-neonatal airway, and who could perform an ex-utero intrapartum treatment to secure the airway. Even after birth, the airway remains central in the patient's overall management. Signs and symptoms of airway compromise must be evaluated keeping in mind the specific requirements of infants and small children and being aware that rapid worsening may occur. The treatment is then tailored to the patient and his lesion with the goal of improving symptoms while avoiding treatment-related complications. Maintaining reasonable expectations by the patient and families are part of a successful management. Cure is achievable for small and localized lesions, but symptom relief and mitigation of functional, esthetic and psychological impairments is the goal for large and complex lesions. If a tracheotomy was required, decannulation is one of the primary management goals.
Keywords: airway management; lymphatic malformation; pediatric airway; subglottic hemangioma; tracheotomy; vascular anomaly; vascular malformation; vascular tumor.
© 2022 The Authors. Journal of Oral Pathology & Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
None.
Figures

Similar articles
-
Current airway management in craniofacial anomalies.Curr Opin Otolaryngol Head Neck Surg. 2003 Dec;11(6):428-32. doi: 10.1097/00020840-200312000-00004. Curr Opin Otolaryngol Head Neck Surg. 2003. PMID: 14631174 Review.
-
Management of the critical airway when an EXIT procedure is not an option: A case report.Int J Pediatr Otorhinolaryngol. 2015 Dec;79(12):2433-7. doi: 10.1016/j.ijporl.2015.08.044. Epub 2015 Sep 10. Int J Pediatr Otorhinolaryngol. 2015. PMID: 26429602
-
Airway management in children with major craniofacial anomalies.Laryngoscope. 1998 Dec;108(12):1806-12. doi: 10.1097/00005537-199812000-00008. Laryngoscope. 1998. PMID: 9851495
-
Fetal surgery in otolaryngology: a new era in the diagnosis and management of fetal airway obstruction because of advances in prenatal imaging.Arch Otolaryngol Head Neck Surg. 2005 May;131(5):393-8. doi: 10.1001/archotol.131.5.393. Arch Otolaryngol Head Neck Surg. 2005. PMID: 15897417
-
Special considerations in vascular anomalies: airway management.Clin Plast Surg. 2011 Jan;38(1):121-31. doi: 10.1016/j.cps.2010.08.008. Clin Plast Surg. 2011. PMID: 21095477 Review.
Cited by
-
General anesthesia for cesarean section in a pregnant woman with systemic vascular malformation: a case report.JA Clin Rep. 2023 Dec 14;9(1):88. doi: 10.1186/s40981-023-00682-0. JA Clin Rep. 2023. PMID: 38095776 Free PMC article.
References
-
- International Society for the Study of Vascular Anomalies . https://www.issva.org/classification. Published 2018.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
