

The Role of Gut-Liver Axis in Gut Microbiome Dysbiosis Associated NAFLD and NAFLD-HCC
- PMID: 35327326
- PMCID: PMC8945287
- DOI: 10.3390/biomedicines10030524
The Role of Gut-Liver Axis in Gut Microbiome Dysbiosis Associated NAFLD and NAFLD-HCC
Abstract
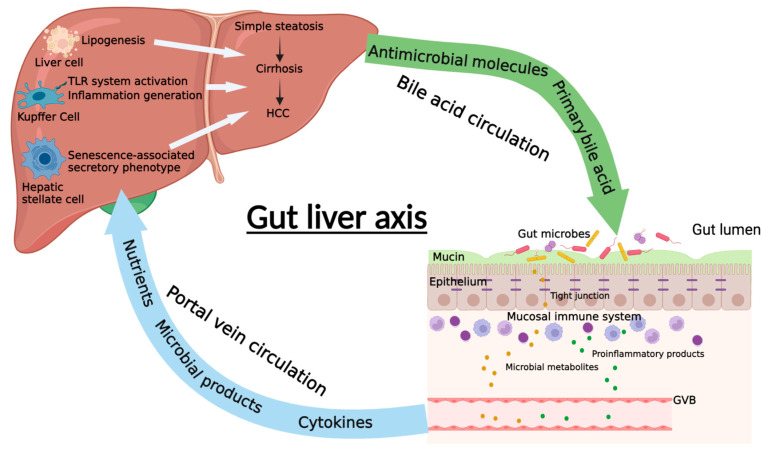
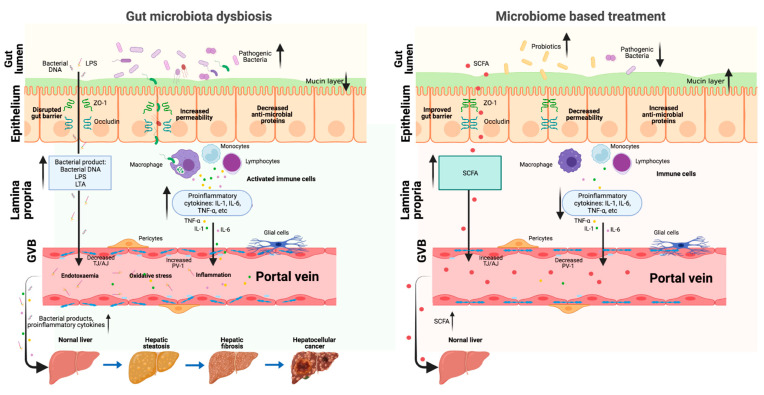
Nonalcoholic fatty liver disease (NAFLD) is considered as one of the most prevalent chronic liver diseases worldwide due to the rapidly rising prevalence of obesity and metabolic syndrome. As a hepatic manifestation of metabolic disease, NAFLD begins with hepatic fat accumulation and progresses to hepatic inflammation, termed as non-alcoholic steatohepatitis (NASH), hepatic fibrosis/cirrhosis, and finally leading to NAFLD-related hepatocellular carcinoma (NAFLD-HCC). Accumulating evidence showed that the gut microbiome plays a vital role in the initiation and progression of NAFLD through the gut-liver axis. The gut-liver axis is the mutual communication between gut and liver comprising the portal circulation, bile duct, and systematic circulation. The gut microbiome dysbiosis contributes to NAFLD development by dysregulating the gut-liver axis, leading to increased intestinal permeability and unrestrained transfer of microbial metabolites into the liver. In this review, we systematically summarized the up-to-date information of gut microbiome dysbiosis and metabolomic changes along the stages of steatosis, NASH, fibrosis, and NAFLD-HCC. The components and functions of the gut-liver axis and its association with NAFLD were then discussed. In addition, we highlighted current knowledge of gut microbiome-based treatment strategies targeting the gut-liver axis for preventing NAFLD and its associated HCC.
Keywords: gut microbiome; gut–liver axis; intestinal barrier; metabolites; non-alcoholic fatty liver disease.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
Similar articles
-
Gut-Liver Axis and Non-Alcoholic Fatty Liver Disease: A Vicious Circle of Dysfunctions Orchestrated by the Gut Microbiome.Biology (Basel). 2022 Nov 6;11(11):1622. doi: 10.3390/biology11111622. Biology (Basel). 2022. PMID: 36358323 Free PMC article. Review.
-
Understanding the Role of the Gut Microbiome and Microbial Metabolites in Non-Alcoholic Fatty Liver Disease: Current Evidence and Perspectives.Biomolecules. 2021 Dec 31;12(1):56. doi: 10.3390/biom12010056. Biomolecules. 2021. PMID: 35053205 Free PMC article. Review.
-
Diet and gut microbiome in fatty liver and its associated liver cancer.J Gastroenterol Hepatol. 2022 Jan;37(1):7-14. doi: 10.1111/jgh.15713. Epub 2021 Nov 3. J Gastroenterol Hepatol. 2022. PMID: 34664301 Review.
-
Periodontal treatment and microbiome-targeted therapy in management of periodontitis-related nonalcoholic fatty liver disease with oral and gut dysbiosis.World J Gastroenterol. 2023 Feb 14;29(6):967-996. doi: 10.3748/wjg.v29.i6.967. World J Gastroenterol. 2023. PMID: 36844143 Free PMC article. Review.
-
Molecular Mechanisms: Connections between Nonalcoholic Fatty Liver Disease, Steatohepatitis and Hepatocellular Carcinoma.Int J Mol Sci. 2020 Feb 23;21(4):1525. doi: 10.3390/ijms21041525. Int J Mol Sci. 2020. PMID: 32102237 Free PMC article. Review.
Cited by
-
Systemic impacts of metabolic dysfunction-associated steatotic liver disease (MASLD) and metabolic dysfunction-associated steatohepatitis (MASH) on heart, muscle, and kidney related diseases.Front Cell Dev Biol. 2024 Jul 16;12:1433857. doi: 10.3389/fcell.2024.1433857. eCollection 2024. Front Cell Dev Biol. 2024. PMID: 39086662 Free PMC article. Review.
-
From Reductionistic Approach to Systems Immunology Approach for the Understanding of Tumor Microenvironment.Int J Mol Sci. 2023 Jul 28;24(15):12086. doi: 10.3390/ijms241512086. Int J Mol Sci. 2023. PMID: 37569461 Free PMC article. Review.
-
Long COVID-19 Pathophysiology: What Do We Know So Far?Microorganisms. 2023 Sep 30;11(10):2458. doi: 10.3390/microorganisms11102458. Microorganisms. 2023. PMID: 37894116 Free PMC article. Review.
-
Gut-Liver Axis and Non-Alcoholic Fatty Liver Disease: A Vicious Circle of Dysfunctions Orchestrated by the Gut Microbiome.Biology (Basel). 2022 Nov 6;11(11):1622. doi: 10.3390/biology11111622. Biology (Basel). 2022. PMID: 36358323 Free PMC article. Review.
-
Research Progress of Fecal Microbiota Transplantation in Liver Diseases.J Clin Med. 2023 Feb 20;12(4):1683. doi: 10.3390/jcm12041683. J Clin Med. 2023. PMID: 36836218 Free PMC article. Review.
References
-
- Blond E., Disse E., Cuerq C., Drai J., Valette P.-J., Laville M., Thivolet C., Simon C., Caussy C. EASL–EASD–EASO clinical practice guidelines for the management of non-alcoholic fatty liver disease in severely obese people: Do they lead to over-referral? Diabetologia. 2017;60:1218–1222. doi: 10.1007/s00125-017-4264-9. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
