

Association of Unit Census with Delays in Antimicrobial Initiation among Ward Patients with Hospital-acquired Sepsis
- PMID: 35312462
- PMCID: PMC9447380
- DOI: 10.1513/AnnalsATS.202112-1360OC
Association of Unit Census with Delays in Antimicrobial Initiation among Ward Patients with Hospital-acquired Sepsis
Abstract
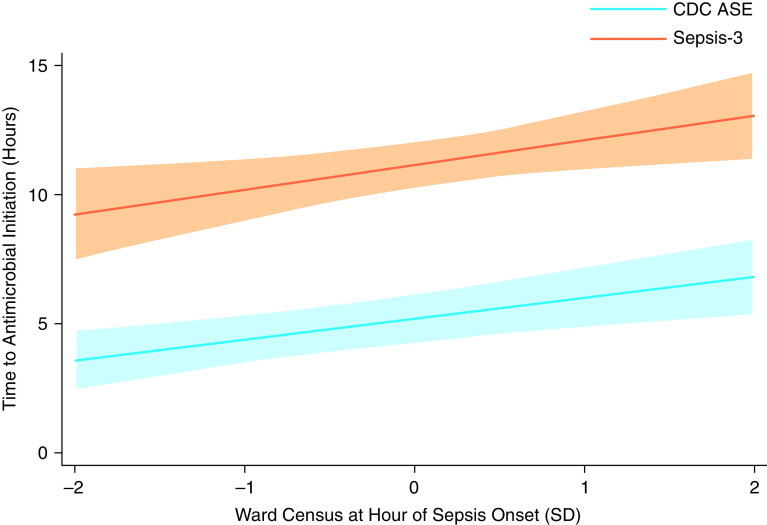
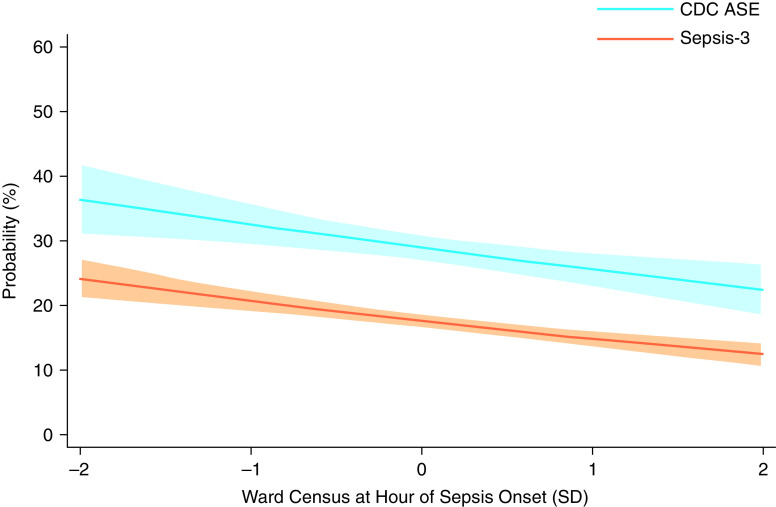
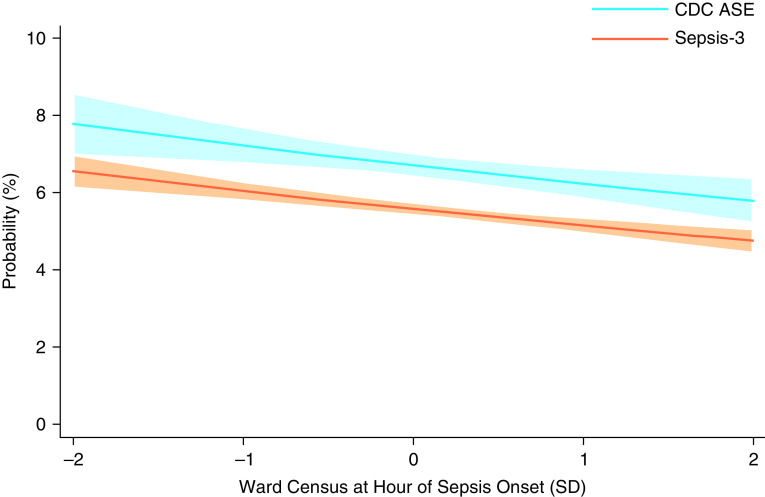
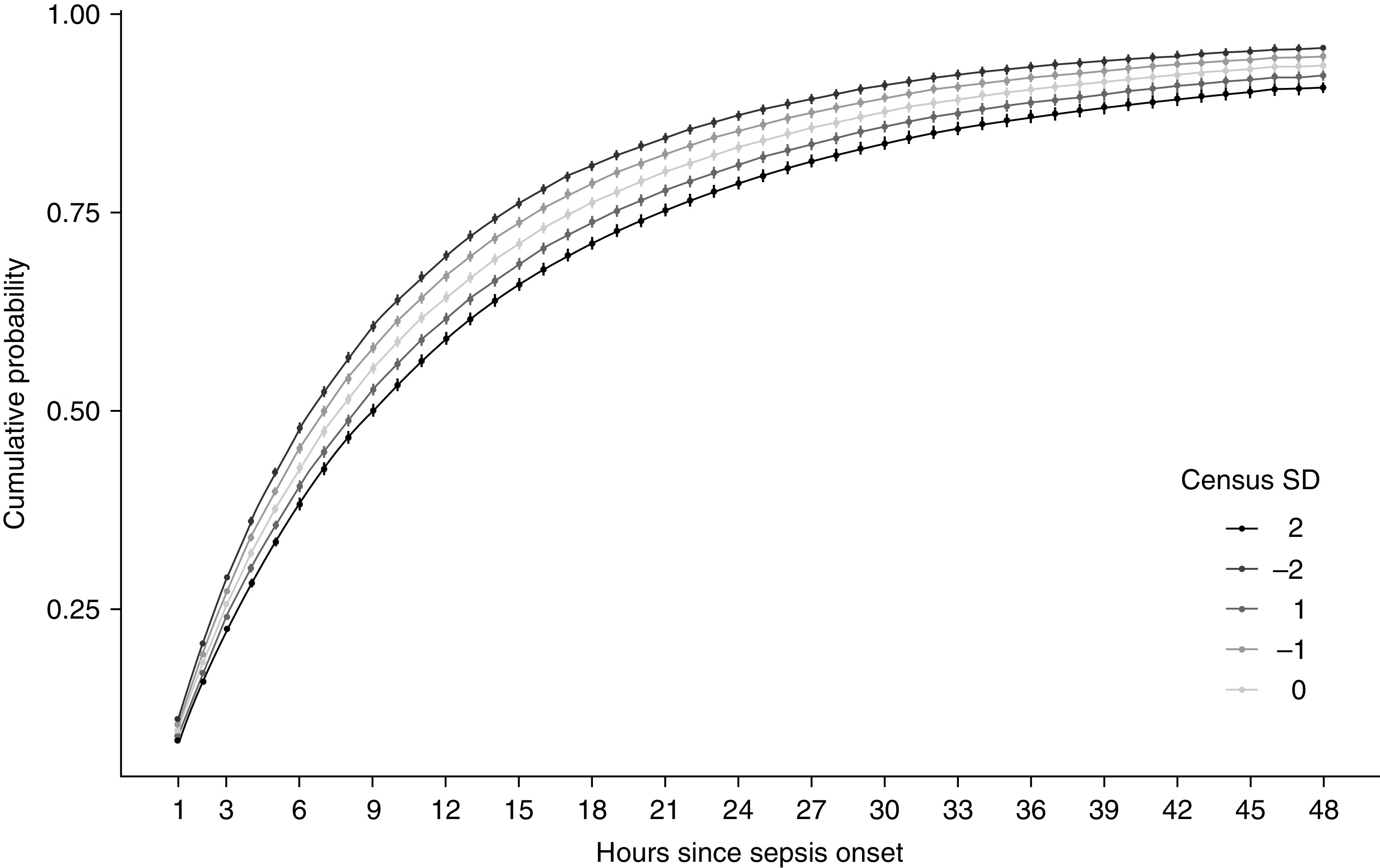
Rationale: Patients with hospital-acquired sepsis (HAS) experience higher mortality and delayed care compared with those with community-acquired sepsis. Capacity strain, the extent to which demand for hospital resources exceeds availability, thus impacting patient care, is a possible mechanism underlying antimicrobial delays for HAS but has not been studied. Objectives: Assess the association of ward census with the timing of antimicrobial initiation among ward patients with HAS. Methods: This retrospective cohort study included adult patients hospitalized at five acute care hospitals between July 2017 and December 2019 who developed ward-onset HAS, distinguished from community-acquired sepsis by onset after 48 hours of hospitalization. The primary exposure was ward census, measured as the number of patients present in each ward at each hour, standardized by quarter and year. The primary outcome was time from sepsis onset to antimicrobial initiation. We used quantile regression to assess the association between ward census at sepsis onset and time to antimicrobial initiation among patients with HAS defined by Centers for Disease Control and Prevention Adult Sepsis Event criteria. We adjusted for hospital, year, quarter, age, sex, race, ethnicity, severity of illness, admission diagnosis, and service type. Results: A total of 1,672 hospitalizations included at least one ward-onset HAS episode. Median time to antimicrobial initiation after HAS onset was 4.1 hours (interquartile range, 0.4-22.3). Marginal adjusted time to antimicrobial initiation ranged from 3.6 hours (95% confidence interval [CI], 2.4-4.8 h) to 6.8 hours (95% CI, 5.3-8.4 h) at census levels 2 standard deviations (SDs) below and above the ward-specific mean, respectively. Each 1-SD increase in ward census at sepsis onset, representing a median of 2.4 patients, was associated with an increase in time to antimicrobial initiation of 0.80 hours (95% CI, 0.32-1.29 h). In sensitivity analyses, results were consistent across severity of illness and electronic health record-based sepsis definitions. Conclusions: Time to antimicrobial initiation increased with increasing census among ward patients with HAS. These findings suggest that delays in care for HAS may be related to ward capacity strain as measured by census. Additional work is needed to validate these findings and identify potential mechanisms operating through clinician behavior and care delivery processes.
Keywords: bed occupancy; clinical decision-making; critical care; risk factors; time-to-treatment.
Figures
Comment in
-
What's Taking So Long? Known Unknowns, Capacity Strain, and Hospital-acquired Sepsis.Ann Am Thorac Soc. 2022 Sep;19(9):1453-1454. doi: 10.1513/AnnalsATS.202206-485ED. Ann Am Thorac Soc. 2022. PMID: 36048123 Free PMC article. No abstract available.
Similar articles
-
Association of Time of Day with Delays in Antimicrobial Initiation among Ward Patients with Hospital-Onset Sepsis.Ann Am Thorac Soc. 2023 Sep;20(9):1299-1308. doi: 10.1513/AnnalsATS.202302-160OC. Ann Am Thorac Soc. 2023. PMID: 37166187 Free PMC article.
-
Associations of Intensive Care Unit Capacity Strain with Disposition and Outcomes of Patients with Sepsis Presenting to the Emergency Department.Ann Am Thorac Soc. 2018 Nov;15(11):1328-1335. doi: 10.1513/AnnalsATS.201804-241OC. Ann Am Thorac Soc. 2018. PMID: 30113865 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Automated monitoring compared to standard care for the early detection of sepsis in critically ill patients.Cochrane Database Syst Rev. 2018 Jun 25;6(6):CD012404. doi: 10.1002/14651858.CD012404.pub2. Cochrane Database Syst Rev. 2018. PMID: 29938790 Free PMC article. Review.
-
Catheter impregnation, coating or bonding for reducing central venous catheter-related infections in adults.Cochrane Database Syst Rev. 2016 Mar 16;3(3):CD007878. doi: 10.1002/14651858.CD007878.pub3. Cochrane Database Syst Rev. 2016. PMID: 26982376 Free PMC article. Review.
Cited by
-
Association of Time of Day with Delays in Antimicrobial Initiation among Ward Patients with Hospital-Onset Sepsis.Ann Am Thorac Soc. 2023 Sep;20(9):1299-1308. doi: 10.1513/AnnalsATS.202302-160OC. Ann Am Thorac Soc. 2023. PMID: 37166187 Free PMC article.
-
What's Taking So Long? Known Unknowns, Capacity Strain, and Hospital-acquired Sepsis.Ann Am Thorac Soc. 2022 Sep;19(9):1453-1454. doi: 10.1513/AnnalsATS.202206-485ED. Ann Am Thorac Soc. 2022. PMID: 36048123 Free PMC article. No abstract available.
-
Effectiveness and Safety of an Emergency Department Code Sepsis Protocol: A Pragmatic Clinical Trial.Ann Am Thorac Soc. 2024 Nov;21(11):1560-1571. doi: 10.1513/AnnalsATS.202403-286OC. Ann Am Thorac Soc. 2024. PMID: 38996086 Free PMC article. Clinical Trial.
-
Hospital-Onset Sepsis Warrants Expanded Investigation and Consideration as a Unique Clinical Entity.Chest. 2024 Jun;165(6):1421-1430. doi: 10.1016/j.chest.2024.01.028. Epub 2024 Jan 19. Chest. 2024. PMID: 38246522 Free PMC article. Review.
References
-
- Rhee C, Wang R, Zhang Z, Fram D, Kadri SS, Klompas M, CDC Prevention Epicenters Program Epidemiology of hospital-onset versus community-onset sepsis in U.S. hospitals and association with mortality: a retrospective analysis using electronic clinical data. Crit Care Med . 2019;47:1169–1176. - PMC - PubMed
-
- Sun A, Netzer G, Small DS, Hanish A, Fuchs BD, Gaieski DF, et al. Association between index hospitalization and hospital readmission in sepsis survivors. Crit Care Med . 2016;44:478–487. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
