

Pharmacokinetics of Caffeine: A Systematic Analysis of Reported Data for Application in Metabolic Phenotyping and Liver Function Testing
- PMID: 35280254
- PMCID: PMC8914174
- DOI: 10.3389/fphar.2021.752826
Pharmacokinetics of Caffeine: A Systematic Analysis of Reported Data for Application in Metabolic Phenotyping and Liver Function Testing
Abstract
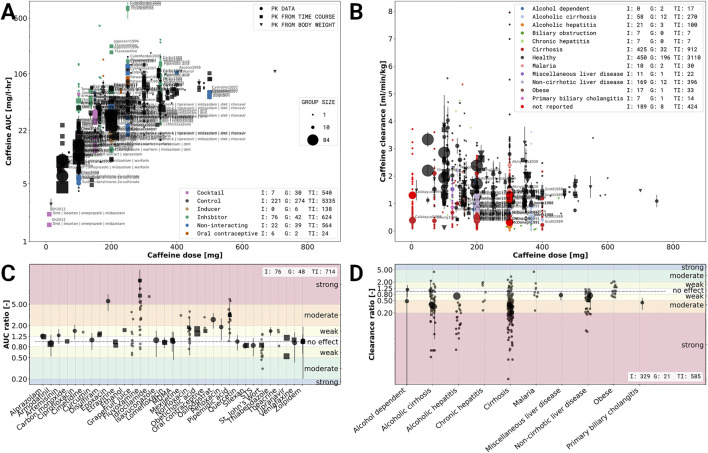
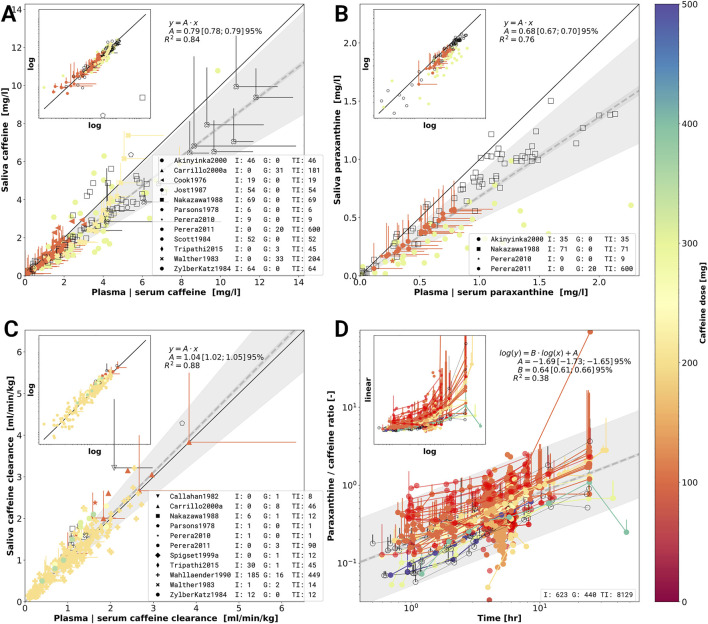
Caffeine is by far the most ubiquitous psychostimulant worldwide found in tea, coffee, cocoa, energy drinks, and many other beverages and food. Caffeine is almost exclusively metabolized in the liver by the cytochrome P-450 enzyme system to the main product paraxanthine and the additional products theobromine and theophylline. Besides its stimulating properties, two important applications of caffeine are metabolic phenotyping of cytochrome P450 1A2 (CYP1A2) and liver function testing. An open challenge in this context is to identify underlying causes of the large inter-individual variability in caffeine pharmacokinetics. Data is urgently needed to understand and quantify confounding factors such as lifestyle (e.g., smoking), the effects of drug-caffeine interactions (e.g., medication metabolized via CYP1A2), and the effect of disease. Here we report the first integrative and systematic analysis of data on caffeine pharmacokinetics from 141 publications and provide a comprehensive high-quality data set on the pharmacokinetics of caffeine, caffeine metabolites, and their metabolic ratios in human adults. The data set is enriched by meta-data on the characteristics of studied patient cohorts and subjects (e.g., age, body weight, smoking status, health status), the applied interventions (e.g., dosing, substance, route of application), measured pharmacokinetic time-courses, and pharmacokinetic parameters (e.g., clearance, half-life, area under the curve). We demonstrate via multiple applications how the data set can be used to solidify existing knowledge and gain new insights relevant for metabolic phenotyping and liver function testing based on caffeine. Specifically, we analyzed 1) the alteration of caffeine pharmacokinetics with smoking and use of oral contraceptives; 2) drug-drug interactions with caffeine as possible confounding factors of caffeine pharmacokinetics or source of adverse effects; 3) alteration of caffeine pharmacokinetics in disease; and 4) the applicability of caffeine as a salivary test substance by comparison of plasma and saliva data. In conclusion, our data set and analyses provide important resources which could enable more accurate caffeine-based metabolic phenotyping and liver function testing.
Keywords: CYP1A2; caffeine; drug-disease interactions; drug-drug interactions; liver function test; oral contraceptives; pharmacokinetics; smoking.
Copyright © 2022 Grzegorzewski, Bartsch , Köller and König.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Paraxanthine/Caffeine Concentration Ratios in Hair: An Alternative for Plasma-Based Phenotyping of Cytochrome P450 1A2?Clin Pharmacokinet. 2015 Jul;54(7):771-81. doi: 10.1007/s40262-015-0237-7. Clin Pharmacokinet. 2015. PMID: 25603821
-
Evaluation of caffeine as a test drug for CYP1A2, NAT2 and CYP2E1 phenotyping in man by in vivo versus in vitro correlations.Pharmacogenetics. 1996 Apr;6(2):159-76. doi: 10.1097/00008571-199604000-00003. Pharmacogenetics. 1996. PMID: 9156694
-
Assessment of CYP1A2 activity in clinical practice: why, how, and when?Basic Clin Pharmacol Toxicol. 2005 Sep;97(3):125-34. doi: 10.1111/j.1742-7843.2005.pto_973160.x. Basic Clin Pharmacol Toxicol. 2005. PMID: 16128905 Review.
-
The effects of acute falciparum malaria on the disposition of caffeine and the comparison of saliva and plasma-derived pharmacokinetic parameters in adult Nigerians.Eur J Clin Pharmacol. 2000 May;56(2):159-65. doi: 10.1007/s002280050735. Eur J Clin Pharmacol. 2000. PMID: 10877011 Clinical Trial.
-
Measurement of CYP1A2 activity: a focus on caffeine as a probe.Curr Drug Metab. 2012 Jun 1;13(5):667-78. doi: 10.2174/1389200211209050667. Curr Drug Metab. 2012. PMID: 22554278 Review.
Cited by
-
Neurodegenerative Diseases: Can Caffeine Be a Powerful Ally to Weaken Neuroinflammation?Int J Mol Sci. 2022 Oct 26;23(21):12958. doi: 10.3390/ijms232112958. Int J Mol Sci. 2022. PMID: 36361750 Free PMC article. Review.
-
The effect of caffeine dose on caffeine and paraxanthine changes in serum and saliva and CYP1A2 enzyme activity in athletes: a randomized placebo-controlled crossover trial.Nutr Metab (Lond). 2024 Nov 11;21(1):90. doi: 10.1186/s12986-024-00863-3. Nutr Metab (Lond). 2024. PMID: 39529054 Free PMC article.
-
A pathway model of glucose-stimulated insulin secretion in the pancreatic β-cell.Front Endocrinol (Lausanne). 2023 Aug 2;14:1185656. doi: 10.3389/fendo.2023.1185656. eCollection 2023. Front Endocrinol (Lausanne). 2023. PMID: 37600713 Free PMC article.
-
Cognitive effects of guarana supplementation with maximal intensity cycling.Br J Nutr. 2023 Jul 28;130(2):253-260. doi: 10.1017/S0007114522002859. Epub 2022 Sep 23. Br J Nutr. 2023. PMID: 36146946 Free PMC article. Clinical Trial.
-
Beyond AOPs: A Mechanistic Evaluation of NAMs in DART Testing.Front Toxicol. 2022 Mar 7;4:838466. doi: 10.3389/ftox.2022.838466. eCollection 2022. Front Toxicol. 2022. PMID: 35295212 Free PMC article.
References
-
- Akinyinka O. O., Sowunmi A., Honeywell R., Renwick A. G. (2000). The Effects of Acute Falciparum Malaria on the Disposition of Caffeine and the Comparison of Saliva and Plasma-Derived Pharmacokinetic Parameters in Adult Nigerians. Eur. J. Clin. Pharmacol. 56, 159–165. 10.1007/s002280050735 - DOI - PubMed
-
- Amchin J., Zarycranski W., Taylor K. P., Albano D., Klockowski P. M. (1999). Effect of Venlafaxine on Cyp1a2-dependent Pharmacokinetics and Metabolism of Caffeine. J. Clin. Pharmacol. 39, 252–259. - PubMed
-
- Armani S., Ting L., Sauter N., Darstein C., Tripathi A. P., Wang L., et al. (2017). Drug Interaction Potential of Osilodrostat (Lci699) Based on its Effect on the Pharmacokinetics of Probe Drugs of Cytochrome P450 Enzymes in Healthy Adults. Clin. Drug Investig. 37, 465–472. 10.1007/s40261-017-0497-0 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources