

Genomic Epidemiology Suggests Community Origins of Healthcare-Associated USA300 Methicillin-Resistant Staphylococcus aureus
- PMID: 35172338
- PMCID: PMC9612791
- DOI: 10.1093/infdis/jiac056
Genomic Epidemiology Suggests Community Origins of Healthcare-Associated USA300 Methicillin-Resistant Staphylococcus aureus
Abstract
Background: Hospital-onset (HO) methicillin-resistant Staphylococcus aureus (MRSA) infections have declined over the past decade due to infection control strategies; community-onset (CO) and healthcare-associated community-onset (HACO) MRSA, particularly USA300, has declined less. We examined the role of community strains to explain the difference.
Methods: We performed whole-genome sequencing (WGS) on MRSA clinical isolates from Cook County Health patients during 2011-2014. We defined infections as CO, HO, or HACO epidemiologically. We integrated genomic, community exposure, and statewide hospital discharge data to infer MRSA origin.
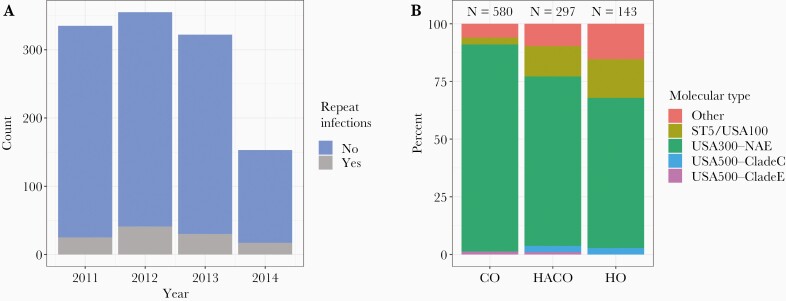
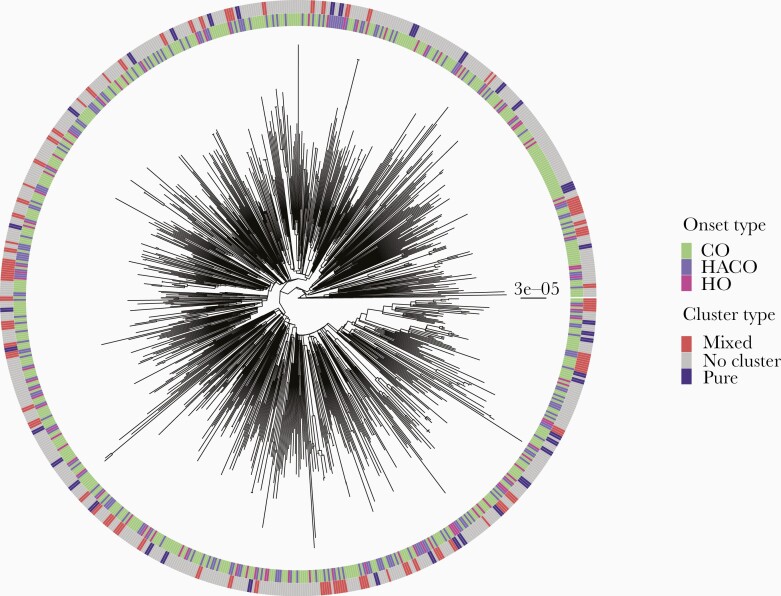
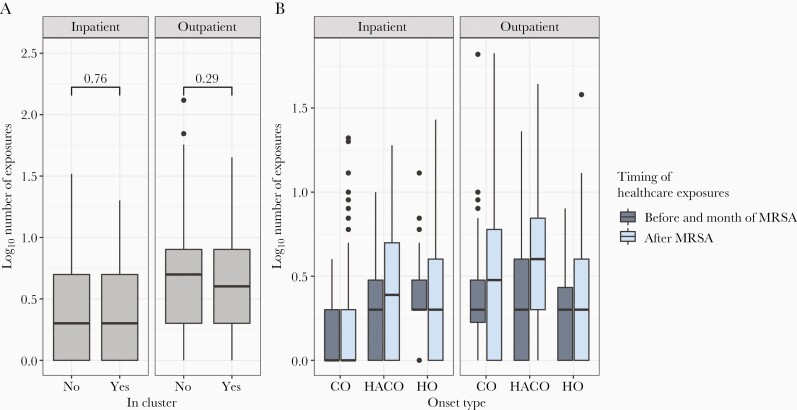
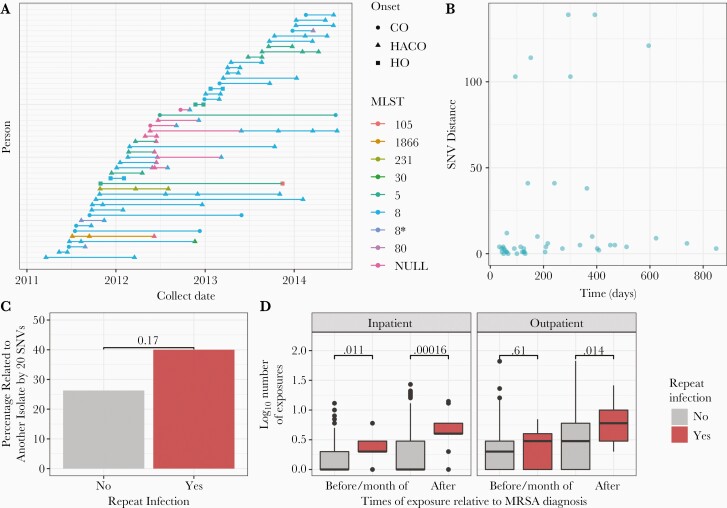
Results: Among 1020 individuals with available WGS, most were USA300 wound infections (580 CO, 143 HO, 297 HACO). USA300 HO, CO, and HACO infections were intermixed on the USA300 phylogeny, consistent with common strains circulating across community and healthcare settings. Community exposures (eg, substance abuse, incarceration, homelessness) were associated with HACO and HO infections, and genetically linked individuals from both groups had little overlap in healthcare facilities, supporting community origins. Most repeat infections-over months to years-occurred in individuals persistently carrying their own strains. These individuals were more likely to have genetic linkages, suggesting a role of persistent colonization in transmission.
Conclusions: Efforts to reduce presumed nosocomial USA300 spread may require understanding and controlling community sources and transmission networks, particularly for repeat infections.
Keywords: MRSA; community transmission; genomic epidemiology; healthcare-associated community-onset; repeat infection.
© The Author(s) 2022. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Conflict of interest statement
Potential conflicts of interest. All authors: No reported conflicts of interest.
Figures
Comment in
-
Community Origins of Health Care-Associated CC59 Methicillin-Resistant Staphylococcus aureus in China.J Infect Dis. 2022 Dec 13;226(12):2238-2239. doi: 10.1093/infdis/jiac212. J Infect Dis. 2022. PMID: 35594904 No abstract available.
Similar articles
-
Genomic Update of Phenotypic Prediction Rule for Methicillin-Resistant Staphylococcus aureus (MRSA) USA300 Discloses Jail Transmission Networks with Increased Resistance.Microbiol Spectr. 2021 Sep 3;9(1):e0037621. doi: 10.1128/Spectrum.00376-21. Epub 2021 Jul 21. Microbiol Spectr. 2021. PMID: 34287060 Free PMC article.
-
Genomic and Epidemiological Evidence for Community Origins of Hospital-Onset Methicillin-Resistant Staphylococcus aureus Bloodstream Infections.J Infect Dis. 2017 Jun 1;215(11):1640-1647. doi: 10.1093/infdis/jiw647. J Infect Dis. 2017. PMID: 28486667 Free PMC article.
-
Epidemiology of healthcare-associated bloodstream infection caused by USA300 strains of methicillin-resistant Staphylococcus aureus in 3 affiliated hospitals.Infect Control Hosp Epidemiol. 2009 Mar;30(3):233-41. doi: 10.1086/595963. Infect Control Hosp Epidemiol. 2009. PMID: 19199535
-
Global epidemiology of community-associated methicillin resistant Staphylococcus aureus (CA-MRSA).Curr Opin Microbiol. 2012 Oct;15(5):588-95. doi: 10.1016/j.mib.2012.08.003. Epub 2012 Oct 5. Curr Opin Microbiol. 2012. PMID: 23044073 Review.
-
Community-associated meticillin-resistant Staphylococcus aureus strains as a cause of healthcare-associated infection.J Hosp Infect. 2011 Nov;79(3):189-93. doi: 10.1016/j.jhin.2011.04.028. Epub 2011 Jul 7. J Hosp Infect. 2011. PMID: 21741111 Review.
Cited by
-
Strain Differences in Bloodstream and Skin Infection: Methicillin-Resistant Staphylococcus aureus Isolated in 2018-2021 in a Single Health System.Open Forum Infect Dis. 2024 May 6;11(6):ofae261. doi: 10.1093/ofid/ofae261. eCollection 2024 Jun. Open Forum Infect Dis. 2024. PMID: 38854395 Free PMC article.
-
Progress in the Prevalence, Classification and Drug Resistance Mechanisms of Methicillin-Resistant Staphylococcus aureus.Infect Drug Resist. 2023 May 25;16:3271-3292. doi: 10.2147/IDR.S412308. eCollection 2023. Infect Drug Resist. 2023. PMID: 37255882 Free PMC article. Review.
-
Infectious Diseases Among People Experiencing Homelessness: A Systematic Review of the Literature in the United States and Canada, 2003-2022.Public Health Rep. 2024 Sep-Oct;139(5):532-548. doi: 10.1177/00333549241228525. Epub 2024 Feb 20. Public Health Rep. 2024. PMID: 38379269 Review.
-
Different evolution of S. aureus methicillin-resistant and methicillin-susceptible infections, Argentina.Heliyon. 2023 Nov 25;10(1):e22610. doi: 10.1016/j.heliyon.2023.e22610. eCollection 2024 Jan 15. Heliyon. 2023. PMID: 38163174 Free PMC article.
-
Clonal Diversity, Antibiotic Resistance, and Virulence Factor Prevalence of Community Associated Staphylococcus aureus in Southeastern Virginia.Pathogens. 2023 Dec 27;13(1):25. doi: 10.3390/pathogens13010025. Pathogens. 2023. PMID: 38251333 Free PMC article.
References
-
- Fridkin SK, Hageman JC, Morrison M, et al. . Methicillin-resistant Staphylococcus aureus disease in three communities. N Engl J Med 2005; 352:1436–44. - PubMed
-
- Centers for Disease Control and Prevention. Methicillin-resistant Staphylococcus aureus infections in correctional facilities—Georgia, California, and Texas, 2001-2003. MMWR Morb Mortal Wkly Rep 2003; 52:992–6. - PubMed
-
- Centers for Disease Control and Prevention. Methicillin-resistant Staphylococcus aureus skin or soft tissue infections in a state prison—Mississippi, 2000. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5042a2.htm. Accessed 19 August 2018. - PubMed
-
- Centers for Disease Control and Prevention. Methicillin-resistant Staphylococcus aureus infections among competitive sports participants—Colorado, Indiana, Pennsylvania, and Los Angeles County, 2000–2003. https://www.cdc.gov/mmwr/preview/mmwrhtml/mm5233a4.htm. Accessed 19 August 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
