

Defining COVID-19-associated pulmonary aspergillosis: systematic review and meta-analysis
- PMID: 35150878
- PMCID: PMC8828380
- DOI: 10.1016/j.cmi.2022.01.027
Defining COVID-19-associated pulmonary aspergillosis: systematic review and meta-analysis
Abstract
Background: Pulmonary aspergillosis may complicate coronavirus disease 2019 (COVID-19) and contribute to excess mortality in intensive care unit (ICU) patients. The disease is poorly understood, in part due to discordant definitions across studies.
Objectives: We sought to review the prevalence, diagnosis, treatment, and outcomes of COVID-19-associated pulmonary aspergillosis (CAPA) and compare research definitions.
Data sources: PubMed, Embase, Web of Science, and MedRxiv were searched from inception to October 12, 2021.
Study eligibility criteria: ICU cohort studies and CAPA case series including ≥3 patients were included.
Participants: Adult patients in ICUs with COVID-19.
Interventions: Patients were reclassified according to four research definitions. We assessed risk of bias with an adaptation of the Joanna Briggs Institute cohort checklist tool for systematic reviews.
Methods: We calculated CAPA prevalence using the Freeman-Tukey random effects method. Correlations between definitions were assessed with Spearman's rank test. Associations between antifungals and outcome were assessed with random effects meta-analysis.
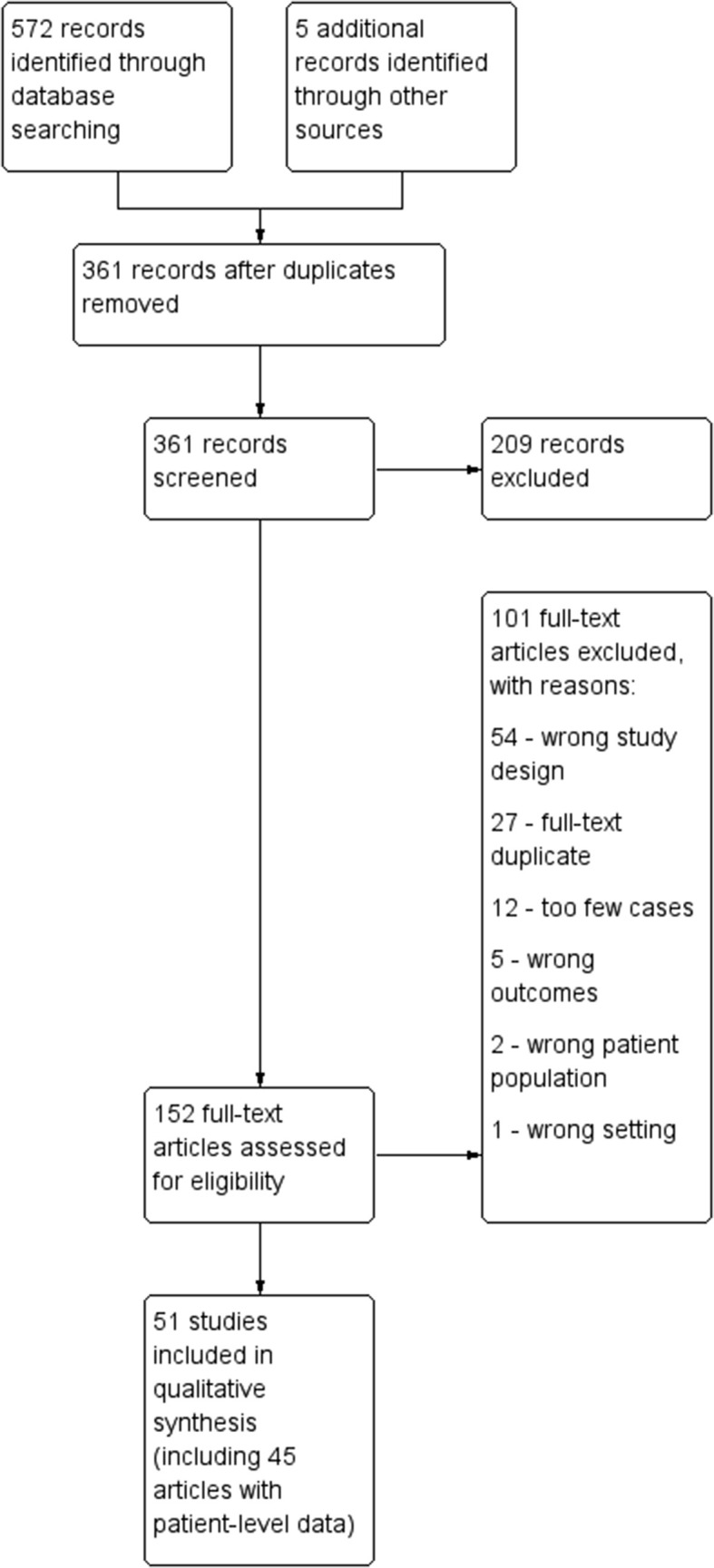
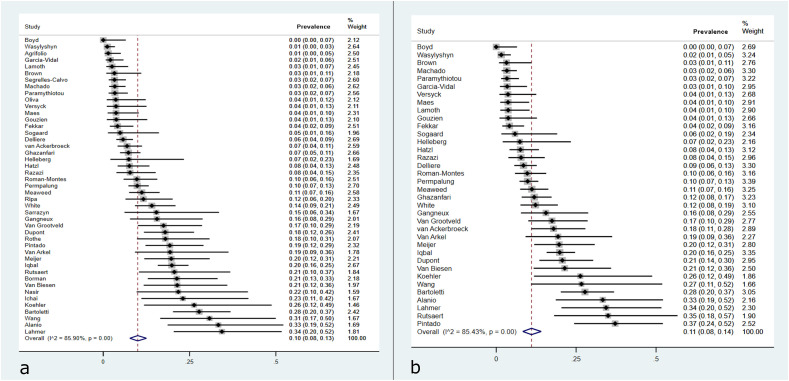
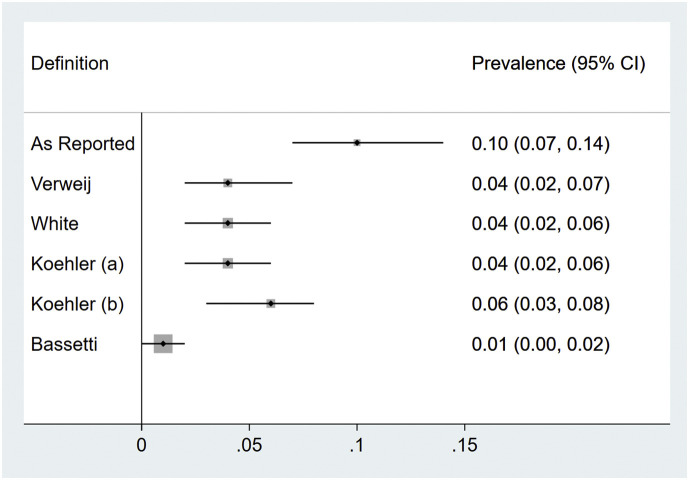
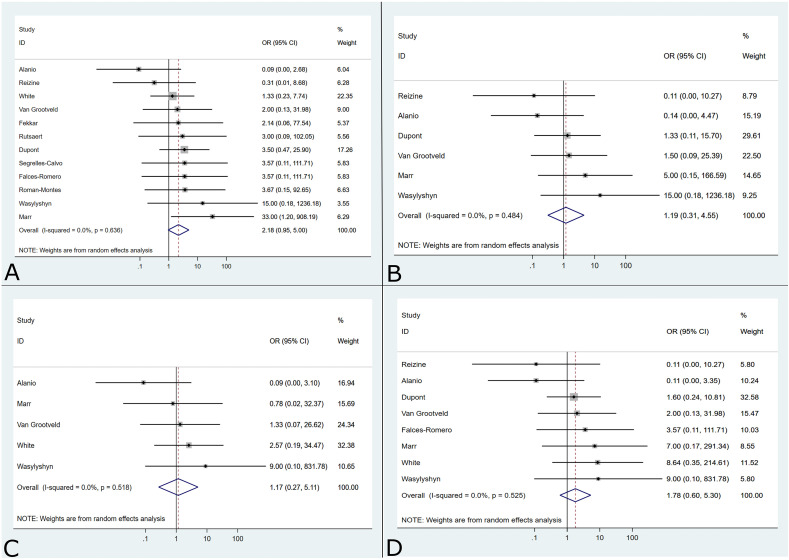
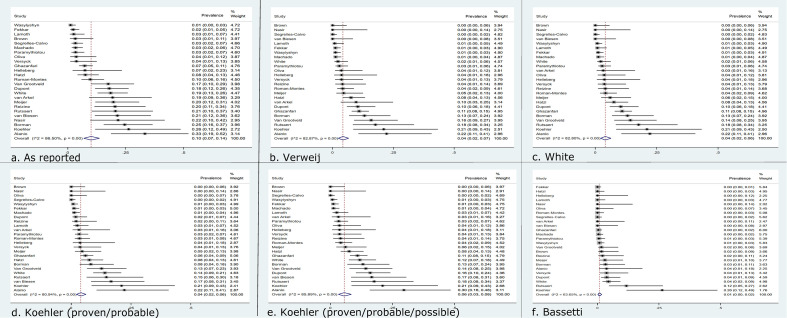
Results: Fifty-one studies were included. Among 3297 COVID-19 patients in ICU cohort studies, 313 were diagnosed with CAPA (prevalence 10%; 95% CI 8%-13%). Two hundred seventy-seven patients had patient-level data allowing reclassification. Definitions had limited correlation with one another (ρ = 0.268-0.447; p < 0.001), with the exception of Koehler and Verweij (ρ = 0.893; p < 0.001); 33.9% of patients reported to have CAPA did not fulfill any research definitions. Patients were diagnosed after a median of 8 days (interquartile range 5-14) in ICUs. Tracheobronchitis occurred in 3% of patients examined with bronchoscopy. The mortality rate was high (59.2%). Applying CAPA research definitions did not strengthen the association between mould-active antifungals and survival.
Conclusions: The reported prevalence of CAPA is significant but may be exaggerated by nonstandard definitions.
Keywords: Aspergillus; CAPA; Fungal infection; ICU; Mycosis; SARS-CoV-2; Secondary infection.
Copyright © 2022 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Figures

Similar articles
-
COVID-19-Associated Pulmonary Aspergillosis, Fungemia, and Pneumocystosis in the Intensive Care Unit: a Retrospective Multicenter Observational Cohort during the First French Pandemic Wave.Microbiol Spectr. 2021 Oct 31;9(2):e0113821. doi: 10.1128/Spectrum.01138-21. Epub 2021 Oct 20. Microbiol Spectr. 2021. PMID: 34668768 Free PMC article.
-
Risk factors and outcome of pulmonary aspergillosis in critically ill coronavirus disease 2019 patients-a multinational observational study by the European Confederation of Medical Mycology.Clin Microbiol Infect. 2022 Apr;28(4):580-587. doi: 10.1016/j.cmi.2021.08.014. Epub 2021 Aug 26. Clin Microbiol Infect. 2022. PMID: 34454093 Free PMC article.
-
Taskforce report on the diagnosis and clinical management of COVID-19 associated pulmonary aspergillosis.Intensive Care Med. 2021 Aug;47(8):819-834. doi: 10.1007/s00134-021-06449-4. Epub 2021 Jun 23. Intensive Care Med. 2021. PMID: 34160631 Free PMC article.
-
Comparing the clinical characteristics and outcomes of COVID-19-associate pulmonary aspergillosis (CAPA): a systematic review and meta-analysis.Infection. 2022 Feb;50(1):43-56. doi: 10.1007/s15010-021-01701-x. Epub 2021 Sep 27. Infection. 2022. PMID: 34570355 Free PMC article. Review.
-
COVID-19-associated pulmonary aspergillosis: an underdiagnosed or overtreated infection?Curr Opin Crit Care. 2022 Oct 1;28(5):470-479. doi: 10.1097/MCC.0000000000000977. Epub 2022 Aug 11. Curr Opin Crit Care. 2022. PMID: 35950729 Free PMC article. Review.
Cited by
-
Renal aspergillosis after COVID-19-associated pulmonary aspergillosis: A case report.Clin Case Rep. 2023 Sep 7;11(9):e7882. doi: 10.1002/ccr3.7882. eCollection 2023 Sep. Clin Case Rep. 2023. PMID: 37692155 Free PMC article.
-
Long-Term Follow-Up of Patients Diagnosed with COVID-19-Associated Pulmonary Aspergillosis (CAPA).J Fungi (Basel). 2022 Aug 11;8(8):840. doi: 10.3390/jof8080840. J Fungi (Basel). 2022. PMID: 36012828 Free PMC article.
-
Meningeal cryptococcosis and SARS-CoV-2 infection in people living with HIV/AIDS.Biomedica. 2023 Aug 31;43(Sp. 1):206-216. doi: 10.7705/biomedica.6872. Biomedica. 2023. PMID: 37721913 Free PMC article.
-
Incidence and inhospital outcomes of coronavirus disease 2019-associated pulmonary aspergillosis in the United States.Ann Thorac Med. 2024 Jan-Mar;19(1):87-95. doi: 10.4103/atm.atm_190_23. Epub 2024 Jan 25. Ann Thorac Med. 2024. PMID: 38444990 Free PMC article.
-
Incidence and Mortality of COVID-19-Associated Invasive Fungal Infections Among Critically Ill Intubated Patients: A Multicenter Retrospective Cohort Analysis.Open Forum Infect Dis. 2024 Apr 2;11(4):ofae108. doi: 10.1093/ofid/ofae108. eCollection 2024 Apr. Open Forum Infect Dis. 2024. PMID: 38567199 Free PMC article.
References
-
- Schauwvlieghe A.F.A.D., Rijnders B.J.A., Philips N., Verwijs R., Vanderbeke L., Van Tienen C., et al. Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir Med. 2018;6:782–792. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
