

Role and Mechanism of the Renin-Angiotensin-Aldosterone System in the Onset and Development of Cardiorenal Syndrome
- PMID: 35111237
- PMCID: PMC8803448
- DOI: 10.1155/2022/3239057
Role and Mechanism of the Renin-Angiotensin-Aldosterone System in the Onset and Development of Cardiorenal Syndrome
Abstract
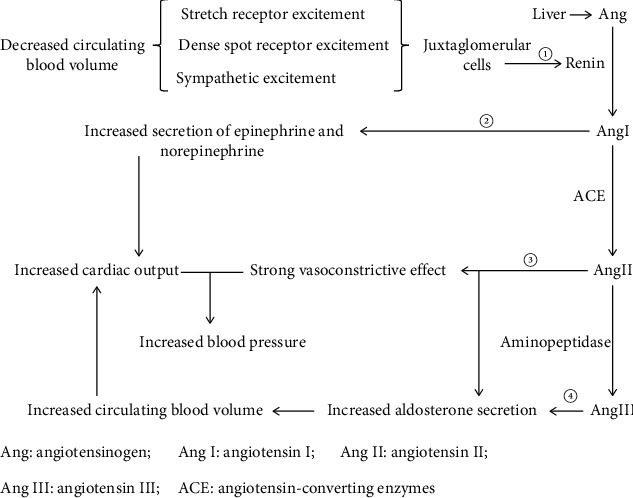
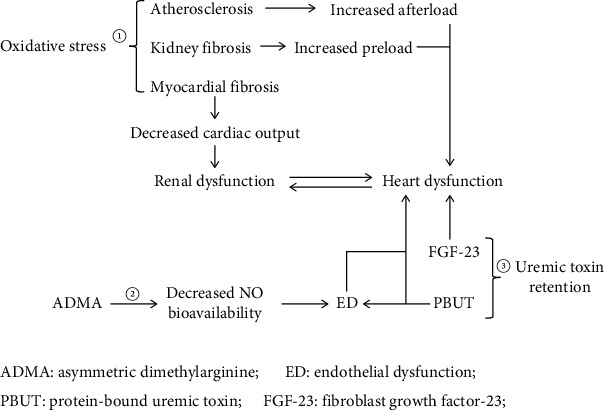
Cardiorenal syndrome (CRS), a clinical syndrome involving multiple pathological mechanisms, exhibits high morbidity and mortality. According to the primary activity of the disease, CRS can be divided into cardiorenal syndrome (type I and type II), renal heart syndrome (type III and type IV), and secondary heart and kidney disease (type V). The renin-angiotensin-aldosterone system (RAAS) is an important humoral regulatory system of the body that exists widely in various tissues and organs. As a compensatory mechanism, the RAAS is typically activated to participate in the regulation of target organ function. RAAS activation plays a key role in the pathogenesis of CRS. The RAAS induces the onset and development of CRS by mediating oxidative stress, uremic toxin overload, and asymmetric dimethylarginine production. Research on the mechanism of RAAS-induced CRS can provide multiple intervention methods that are of great significance for reducing end-stage organ damage and further improving the quality of life of patients with CRS.
Copyright © 2022 Kexin Ma et al.
Conflict of interest statement
There is no conflict of interest in the article.
Figures
Similar articles
-
New roles for renin and prorenin in heart failure and cardiorenal crosstalk.Heart Fail Rev. 2012 Mar;17(2):191-201. doi: 10.1007/s10741-011-9262-2. Heart Fail Rev. 2012. PMID: 21695549 Free PMC article. Review.
-
Role of Renal Oxidative Stress in the Pathogenesis of the Cardiorenal Syndrome.Heart Lung Circ. 2016 Aug;25(8):874-80. doi: 10.1016/j.hlc.2016.02.022. Epub 2016 Apr 16. Heart Lung Circ. 2016. PMID: 27132623 Review.
-
Cardiorenal Syndrome and Heart Failure-Challenges and Opportunities.Can J Cardiol. 2019 Sep;35(9):1208-1219. doi: 10.1016/j.cjca.2019.04.002. Epub 2019 Apr 12. Can J Cardiol. 2019. PMID: 31300181 Free PMC article. Review.
-
RAAS inhibition and cardiorenal syndrome.Curr Hypertens Rev. 2014;10(2):107-11. doi: 10.2174/1573402111666141231144228. Curr Hypertens Rev. 2014. PMID: 25549841 Review.
-
Cardiorenal syndrome: long road between kidney and heart.Heart Fail Rev. 2022 Nov;27(6):2137-2153. doi: 10.1007/s10741-022-10218-w. Epub 2022 Feb 8. Heart Fail Rev. 2022. PMID: 35133552 Review.
Cited by
-
Organ Crosstalk in Acute Kidney Injury: Evidence and Mechanisms.J Clin Med. 2022 Nov 9;11(22):6637. doi: 10.3390/jcm11226637. J Clin Med. 2022. PMID: 36431113 Free PMC article. Review.
-
Unraveling the Mechanisms of Magnesium Supplementation in Alleviating Chronic Kidney Disease Complications and Progression: Balancing Risks and Benefits.Biol Trace Elem Res. 2024 Sep 10. doi: 10.1007/s12011-024-04368-1. Online ahead of print. Biol Trace Elem Res. 2024. PMID: 39256329 Review.
-
Angiotensin-Converting Enzyme and Renin-Inhibitory Activities of Protein Hydrolysates Produced by Alcalase Hydrolysis of Peanut Protein.Int J Mol Sci. 2024 Jul 7;25(13):7463. doi: 10.3390/ijms25137463. Int J Mol Sci. 2024. PMID: 39000571 Free PMC article.
-
A comprehensive review of acute cardio-renal syndrome: need for novel biomarkers.Front Pharmacol. 2023 May 23;14:1152055. doi: 10.3389/fphar.2023.1152055. eCollection 2023. Front Pharmacol. 2023. PMID: 37288107 Free PMC article. Review.
-
Could Repeated Cardio-Renal Injury Trigger Late Cardiovascular Sequelae in Extreme Endurance Athletes?Sports Med. 2022 Dec;52(12):2821-2836. doi: 10.1007/s40279-022-01734-8. Epub 2022 Jul 18. Sports Med. 2022. PMID: 35851948 Free PMC article. Review.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials